Tennis elbow, also called lateral epicondylitis, is an inflammation of the lateral (outside) bony protuberance at the elbow. It is at this protuberance that the tendon of the long muscles of the hand, wrist and forearm attach to the bone. As the muscles repeatedly and forcefully contract, they pull on the bone, causing inflammation. The trauma is irritating when working the muscles in an awkward position with poor leverage like hitting a backhand in tennis.
It is not unusual for a patient to come to my office with severe pain on the outside of their elbow. Especially, after intensifying their tennis workouts or changing the racquet string tension. Others come to me with pain on the inside of the elbow (“golfer’s elbow”) from wrist action that advanced golfer’s use at impact. However, this problem is not only for tennis players and golfers. Laborers working with wrenches or screwdrivers with an awkward or extended arm can also develop tennis elbow. Others who are vulnerable are: those working for hours at a computer using a mouse as well as those working hard maintaining their lawns and gardens.
In a more chronic problem, lateral elbow pain may arise by a degenerative condition of the tendon fibers on the bony prominence at the lateral elbow. Sporadic scar tissue forms from a poor attempt by the body to overcompensate and heal without eliminating the cause.
While symptoms may vary, pain on the outside of the elbow is almost universal. Patients also report severe burning pain that begins slowly and worsens over time when lifting, gripping or using fingers repetitively. In more severe cases, pain can radiate down the forearm.
Conservative treatment is almost always the first option and is successful in 85-90 percent of patients with tennis elbow. Your physician may prescribe anti-inflammatory medication (over the counter or prescribed). Physical/Occupational therapy, rest, ice, and a tennis elbow brace to protect and rest may be advised. Ergonomic changes in equipment, tools, technique and work-station may be necessary. Improvement should occur in 4-6 weeks. If not, a corticosteroid injection may be needed to apply the medication directly to the inflamed area. Physical therapy, range of motion, and stretching exercises may be necessary prior to a gradual return to activity. Deep friction massage can assist healing.

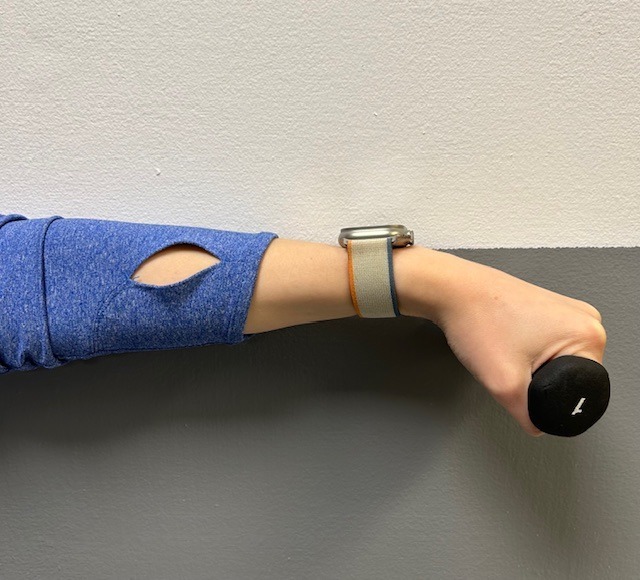
Exercises performed in a particular manner to isometrically hold and eccentrically lengthen the muscle with contraction.
New Conservative Treatment: Platelet-Rich-Plasma (PRP) is a new treatment for the conservative management of degenerated soft tissues that has recently received great media attention. In great part, due to its success in several high profile athletes. According to the Journal of the American Academy of Orthopaedic Surgeons,(JAAOS), platelet-rich plasma (PRP) is autologous (self-donated) blood with an above normal concentration of platelets. Normal blood contains both red and white blood cells, platelets and plasma. Platelets promote the production and revitalization of connective tissue by way of various growth factors on both a chemical and cellular level.
The actual PRP injection requires the patient to donate a small amount of their own blood. The blood is placed into a centrifuge (a machine that spins the blood at a high velocity to separate the different components of blood such as plasma, white and red blood cells), for approximately 15 minutes. Once separated, the physician draws the platelet-rich plasma to be injected directly into the damaged tissue. In theory, the high concentration of platelets, with its inherent ability to stimulate growth and regeneration of connective tissue, will promote and expedite healing.
Surgery for tennis elbow is only considered in patients with severe pain for longer than 6 months without improvement from conservative treatment. One surgical technique involves removing the degenerated portion of the tendon and reattaching the healthy tendon to bone. Recently, arthroscopic surgery developed to perform this technique. However, research does not support the value of one over the other at this point. Physical/occupational therapy is used after surgery. Return to work or athletics may require 4-6 months. More recently, a surgical technique using ultrasound to guide a needle to debride (clean) the area of scar tissue has been developed. If eligible for this procedure, the time required for healing, rehabilitation and return to activity is much shorter.
If you feel you suffer from tennis elbow, ask your family physician which of these treatment options are best for you.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy

This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is repeated every year at this time with the intent of raising the level of awareness to prevent death or serious illness from heat stroke in athletes and other active people in hot, humid weather.
It is the end of July and we have managed to survive two “heat waves” in NEPA. While it is important to have fun in the sun, please be mindful of how your body reacts to high humidity and heat and take appropriate precautions. Athletes are particularly vulnerable this time of year due to daytime practice sessions. (August 5 & 6, 2024, first day of acclimatization and August 12, 2024, first day of practice for fall sports according to PIAA). Visit www.piaa.org for more information. Keep in mind, you don’t have to be running a marathon or playing football in full uniform to suffer from heat stroke.
Heat stroke, one of the most serious heat-related illnesses, is the result of long term exposure to the sun to the point which a person cannot sweat enough to lower the body temperature. The elderly and infants are most susceptible and it can be fatal if not managed properly and immediately. Believe it or not, the exact cause of heatstroke is unclear. Prevention is the best treatment because it can strike suddenly and without warning. It can also occur in non athletes at outdoor concerts, outdoor carnivals, or backyard activities.
Some “old school” folks think that wearing extra clothing and “breaking a good sweat” is an optimal goal for exercise. However, it may be potentially very dangerous in hot and humid conditions. When exercising in hot weather, the body is under additional stress. As the activity and the hot air increases your core temperature your body will to deliver more blood to your skin to cool it down. In doing so, your heart rate is increased and less blood is available for your muscles, which leads to cramping and other more serious problems. In humid conditions, problems are magnified as sweat cannot be evaporated from the skin to assist in cooling the body.
The American Academy of Pediatrics and The American College of Sports Medicine has the following recommendations which are appropriate for both the competitive athlete and weekend warrior:
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Spring is here! So, too, is allergy season and spring sports! It seems this every year at this time a young little league baseball player wheezes as they cross home plate and desperately tries to catch their breath. Players, coaches, umpires, parents watch in dismay, deciding whether they need to call an ambulance. Minutes later the player recovers from this scary situation…until the next time. Could this be an example of exercised-induced asthma (EIA)?
Dr. Gregory Cali, a local pulmonologist, (lung doctor) was gracious enough to participate in an interview about this problem…exercise-induced asthma (EIA). The topic was chosen in response to an email question from a concerned mother of an athlete with asthma. Dr. Cali informed me that the first thing to know about exercise induced asthma (EIA) is that EIA is not a distinct disease in itself-but is one manifestation or presentation of asthma. Putting it simply, EIA occurs in patients who have develop narrowing of the bronchial tubes ( bronchoconstriction) when they exercise. Some experts would rather we use the phrase exercise induced bronchoconstriction which is what happens when someone has an asthma attack. This bronchoconstriction occurs because of spasm of the tiny muscles of the airways, plugging of the airways with thick mucous, and swelling or edema of the cells lining the airways.
In fact, it is inflammation of the airways, mostly due to allergies, that is at the root of most cases of asthma. This inflammation causes the bronchial tubes to become over-reactive-and predisposed to narrowing- when exposed to certain triggers. Exercise is one of those triggers in susceptible people. The patient with EIA complains of chest tightness, wheezing, and shortness of breath when exercising. Some patients only experience coughing with exercise. Symptoms are usually worse in cold, dry air. This is believed to be due to the drying and cooling of the airways, which occurs with exercise, especially if the patient opens his or her mouth while exercising. Nasal breathing is much better at warming and humidifying air and may help to reduce EIA.
Dr. Cali feels that the most important point about EIA is to make sure a specific diagnosis is made. It is difficult at times to differentiate asthma from the normal breathlessness, which occurs with exercise. The feature of EIA that distinguishes it from normal breathing, or being "out of shape" is the fact that EIA is ALWAYS associated with a decrease in airflow. This can be measured with either a peak flow meter or a spirometer. It is also important that a specific diagnosis be made so that a person will not be labeled as asthmatic when they may be "normal" or have other conditions such as heart problems or anemia.
Dr. Cali also recommends before a person is labeled asthmatic, they have spirometric testing. An improvement in airflow after inhaling. A bronchodilator is an important indicator of asthma. Sometimes a bronchial challenge test is needed to diagnose asthma. In this test, the subject breathes in a known bronchoconstrictor in small quantities and the response is noted. Patients with asthma almost always respond to the inhaled agent by a reduction in airflow.
Inform Coaches – If coaches are made aware, than they can be prepared for the onset of EIA. Provide emergency contacts and medications with instructions, such as inhalers, should be available.
Warm and Moisten Air - Whatever the patient can do to warm and moisten the inhaled air can help prevent EIA. Nose breathing during exercise or wearing a loose covering over the mouth in cold weather may help. Sometimes, in severe cases, switching to an indoor sport like swimming may be necessary.
Start Out Slowly - It is important to start out slowly and warm up first before exercising at full tilt. Slowly jog around the track or field before practice or a game to prepare your lungs for full-speed.
Medications – are often necessary. Quick- acting bronchodilators like Albuterol, used 15-20 minutes before planned exercise, is recommended. This can be repeated once more during the exercise, but if tightness or wheezing occurs, the exercise should be stopped. Many patients with asthma require preventative treatment with anti-inflammatory medications. Inhaled steroids and/or leukotriene inhibitors may have to be added if the asthma is not controlled with Albuterol alone. In fact, some patients with asthma who are overly reliant on quick acting bronchodilator medications can get into serious trouble if they do not use inhaled steroids. Be sure to communicate your needs with your coaches.
Play Smart - In conclusion, people with asthma should not shy away from exercise. With proper precautions, people with asthma should be able to participate in all kinds of sports activities: baseball, football, soccer, swimming, tennis and running (even a marathon)! The key point is that the asthma needs to be under control and monitored by the patient, parents, coaches and doctor as a team.
Visit your doctor regularly and listen to your body.
Medical Contributor: Gregory Cali, DO, pulmonary specialist, Dunmore, PA
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is dedicated to the memory of John R. O’Brien, Esq., who recently passed due to medical complications associated with multiple sclerosis (MS). John was a source of joy and inspiration for those fortunate to have known him. Twenty years ago, John hesitantly agreed to contribute to my column on MS with two requirements: one, if the column would be valuable to those affected by MS and two, he would remain anonymous. When speaking with his dedicated wife, Sally, it became very apparent that any discussion of John’s life would be diminished if it was defined by the disease because he was committed to turning his “DISABILITY INTO AN ABILITY!”
With the help of his loving wife, family, friends, and devices such as an electric scooter and adaptive car, John not only lived but thrived! He was a skilled lawyer, a respected member of the Bar, and an active member of the community. John served on the executive committee of the Lackawanna Bar Association. In addition, the Lackawanna Pro Bono honored him recently. He also taught business law and healthcare law and coached Prep’s mock trial team.
John shared his thoughts with me about the challenges of redefining life… from Golf Club Champion to living with a physically disabling disease. Anyone who knew him would agree that he succeeded in doing so through his keen intellect and sharp wit and humor…his heart and brain overcompensated for his body! In addition to reading books in Latin and Greek, he had his crossword puzzles published in The New York Times and Los Angeles Times. In September 2023, John conducted an interview with presidential historian Doris Kearns Goodwin before a full house at the Scranton Cultural Center. Ms. Goodwin later reported that John was the most knowledgeable, effective and enjoyable interviewer she’s encountered.
John’s absence will be deeply felt and his legacy will continue to shape our community for years to come!
Multiple Sclerosis is a chronic disease. While it may lay dormant and stable for a period of time, living a healthy lifestyle will make a positive contribution toward how you and your family live with Multiple Sclerosis. Studies show that a life of family, love, and support are essential to maintain a positive attitude with a chronic illness. This combined with a healthy diet and proper exercise can contribute greatly toward taking control and living a relatively normal life with MS.
As I have mentioned in many other columns, studies show that people with good attitudes and great faith live longer than others. This is especially helpful when living with chronic disease like Multiple Sclerosis. The Cleveland Clinic offers some suggestions how to maintain a positive attitude:
Many sources, including the Cleveland Clinic suggest that exercise, when performed properly, can have a positive impact on Multiple Sclerosis symptoms both physically and psychologically. However, because you have a chronic illness, you should consult with you family physician and physical therapist before beginning an exercise program. They will advise you on the proper type and amount of exercise.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is dedicated to the memory of John R. O’Brien, Esq., who recently passed due to medical complications associated with multiple sclerosis (MS). John was a source of joy and inspiration for those fortunate to have known him. Twenty years ago, John hesitantly agreed to contribute to my column on MS with two requirements: one, if the column would be valuable to those affected by MS and two, he would remain anonymous. When speaking with his dedicated wife, Sally, it became very apparent that any discussion of John’s life would be diminished if it was defined by the disease because he was committed to turning his “DISABILITY INTO AN ABILITY!”
With the help of his loving wife, family, friends, and devices such as an electric scooter and adaptive car, John not only lived but thrived! He was a skilled lawyer, a respected member of the Bar, and an active member of the community. John served on the executive committee of the Lackawanna Bar Association and was recently honored by the Lackawanna Pro Bono. He also taught business law and healthcare law and coached Prep’s mock trial team.
John shared his thoughts with me about the challenges of redefining life… from Golf Club Champion to living with a physically disabling disease. Anyone who knew him would agree that he succeeded in doing so through his keen intellect and sharp wit and humor…his heart and brain overcompensated for his body! In addition to reading books in Latin and Greek, he had his crossword puzzles published in The New York Times and Los Angeles Times. In September 2023, John conducted an interview with presidential historian Doris Kearns Goodwin before a full house at the Scranton Cultural Center. Ms. Goodwin later reported that John was the most knowledgeable, effective and enjoyable interviewer she’s encountered.
John’s absence will be deeply felt and his legacy will continue to shape our community for years to come!
According to the National Multiple Sclerosis Society, Multiple Sclerosis affects approximately 400,000 people in the United States. Multiple Sclerosis is second only to trauma as the most common cause of neurological disability for those in early to middle adulthood. MS is almost three times as common in women. Multiple Sclerosis is very uncommon before adolescence or after 50. However, the risk increases from teen years to age 50.
Multiple sclerosis is considered to be an autoimmune disease. The immune system of the body does not work properly when it fails to attack and protect the body against substances foreign to the body such as bacteria. Instead, the system allows the body to attack normal tissues and create diseases such as MS, rheumatoid arthritis and lupus.
In MS, the immune system attacks the brain and spinal cord of the central nervous system. Each nerve has an outer covering of a fatty material (myelin) for insulation to improve the transmission and conductivity of impulses or messages to and from the brain. The damage to the myelin of the nervous system interrupts the ability of messages to travel to and from the brain, through the spinal cord and to other areas of the body such as the muscles in the arms and legs. Due to this “short circuiting” the brain becomes unable to send or receive messages. In multiple sclerosis, scar tissue or plaques (sclerosis) replaces the fatty myelin in “multiple” areas. This is also called demyelination.
The symptoms associated with MS vary greatly from person to person. The amount, frequency and speed of the demyelination process vary greatly and are directly related to the loss of strength and function in daily activities. Some people are independent and ambulatory with mild and infrequent episodes of weakness and disability and live a relatively normal life. Others suffer from frequent and aggressive episodes that significantly weaken and disable. Some common symptoms in the early stages include: muscle weakness, loss of coordination, blurred vision, pain in the eyes, double vision. Some common symptoms as the disease progresses are: muscle stiffness with muscle spasms, pain, difficulty controlling urination, difficulty thinking clearly.
The diagnosis of MS can be very difficulty in the early stages because the symptoms are often vague and temporary. Also, MS symptoms are very similar to other neurological problems. A neurologist will run several tests to rule out other possible problems. However, an MRI showing demyelination of the nerves is a primary confirmation.
Treatment for MS depends upon many factors and requires consultation with your physician. Some medications can control the frequency and severity of MS symptoms such as pain, weakness, and spasticity. Also, some drugs can slow the progression of certain types of MS. Additional treatments for MS include: diet, exercise, physical therapy, support groups, and counseling for the MS patient and their family. Part II of Multiple Sclerosis will discuss these options in further detail next week.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy - NEXT WEEK: PART II OF II - MULTIPLE SCLEROSIS
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
A myth is a traditional story, idea, or belief, especially one concerning early history of a people or explaining a natural or social phenomenon. It is a widely held but false belief or idea. In medicine, health myths are also widely held beliefs about health issues such as medicines, herbs, treatments, cures, antidotes, etc. which are partially or totally false and unsubstantiated in the scientific literature. This is a partial list of the most common health myths:
SOURCES: WebMd; National Institutes of Health, Mayo Clinic
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article does not intend as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Ice baths have become a new trend or fad in health and fitness, especially among elite athletes and some celebrities. However, it is far from a new treatment modality. In fact, the Ancient Greeks employed cold-water immersion for fever, pain relief, relaxation and socialization. In addition, Hippocrates documented the use of cold for medicinal purposes for its analgesic benefits.
Ice baths, a type of cryotherapy, is also referred to as cold water immersion (CWI) or cold water therapy. This involves immersing your body in ice water for approximately 5-15 minutes from the neck down at 50-59 degrees. The ice baths are commonly used for pain, delayed-onset muscle soreness (DOMS), and inflammation and mood elevation.
In theory, the cold water lowers the temperature of your skin and body by vasoconstriction (narrow) of the blood vessels. When you get out of the cold, water the vasodilatation (widen) of the blood vessels. Immediately, this brings fresh oxygen and nutrient-rich blood back to the tissues to warm the body and in the process, reduce pain, inflammation and promote healing.
If you have the following health conditions, ice baths may not be the best therapeutic modality for you. Before you consider trying an ice bath, consult with your physician to avoid potentially serious problems:
While some studies have shown that subjects report less muscle soreness following CWI when compared to rest, most studies suggest that the reported effects are placebo. Also, reports of improved circulation, reduced inflammation and improved recovery or performance has not been scientifically validated. In view of this, it is recommended that those considering the use of CWI for pain and inflammation management, reduced muscle soreness, and mood elevation, should consult their physician to determine if the potential risks are worth the purported benefits.
SOURCES: nih; health.com; health.clevelandclinic.org; prevention.com
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from many about the nature of the injury and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to “fit in” a warm-up before running or other activities during the winter months. But, no matter how limited time is, skipping the warm-up is risky. This time of year, one can expect to feel a little cold and stiff, especially if you are over 40, and therefore a little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears. The more commonly torn tendon is the Achilles tendon . Prevention of muscle tears, including the Achilles tendon includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions.
A muscle contracts to move bones and joints in the body. The tendon is the fibrous tissue that attaches muscle to bone. Great force is transmitted across a tendon which, in the lower body, can be more than 5 times your body weight. Often, a tendon can become inflamed, irritated, strained or partially torn from improper mechanics or overuse. Although infrequent, occasionally tendons can also snap or rupture. A tendon is more vulnerable to a rupture for several reasons such as a history of repeated injections of steroids into a tendon and use of medications such as corticosteroids and some antibiotics. Certain diseases such as gout, arthritis, diabetes or hyperparathyroidism can contribute to tendon tears. Also, age, obesity and gender are significant risk factors as middle-aged, overweight males are more susceptible to tendon tears. Poor conditioning, improper warm-up and cold temperatures may also contribute to the problem.
Tendon rupture is very painful and debilitating and must not be left untreated. While conservative management is preferred, surgical management is usually required for complete tears. The purpose of this column is to present the signs, symptoms and management of Achilles tendon ruptures.
The Achilles tendon (also called the calcaneal tendon), is a large, strong cordlike band of fibrous tissue in the back of the ankle. The tendon (also called the heel cord) connects the powerful calf muscle to the heel bone (also called the calcaneus). When the calf muscle contracts, (as when you walk on the ball of your foot), the Achilles tendon is tightened, tension is created at the heel and the foot points down like pushing a gas pedal or walking on tip of your toes. This motion is essential for activities such as walking, running, and jumping. A partial tear of the tendon would make these activities weak and painful, while a full tear through the tendon would render these activities impossible.
With age, the Achilles tendon (and other tendons) gets weak, thin, and dehydrated, thus making it prone to inflammation, degeneration, partial tear or rupture. The middle-aged weekend warrior is at greatest risk. A full or complete tear (Achilles tendon rupture) usually occurs about 2 inches above the heel bone and is associated with a sudden burst of activity followed by a quick stop or a quick start or change in direction, as in tennis, racquet ball, and basketball.
In some instances, the tendon can be injured by a violent contraction of calf when you push off forcefully at the same time the knee is locked straight as in a sudden sprint. Other times, the tendon is injured when a sudden and unexpected force occurs as in a trip off a curb or sudden step into a hole or a quick attempt to break a fall.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog Next Week: Achilles tendon Part II of II.
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
November is National Diabetes Awareness Month. This column will present information regarding type 1 and type 2 diabetes and the diagnosis and symptoms of the disease. Next week, Part II will present the role of exercise in the management of the disease.
What is it?
Diabetes is a disease where the hormone insulin is not adequately produced or used by the body. Insulin is needed for cells to take up glucose after it is broken down from sugars, starches and other food that we eat. When working properly, this provides the fuel necessary for activities of daily living. While the exact cause is not completely understood, genetics is known to play a big role. However, environmental factors such as obesity and inactivity have also been found to play a large role.
According to the American Diabetes Association (ADA) and the Centers for Disease Control (CDC), 11.3% of the population in the United States or almost 37.3 million adults and children has diabetes. Unfortunately, the number keeps rising and one-third of these people are not aware that they have the disease.
A Fasting Plasma Glucose Test (FPG) or an Oral Glucose Tolerance Test (OGTT) can be used to screen a person for diabetes or pre-diabetes. Due to the fact that it is easier, quicker and cheaper, the FPG is the recommended test by the ADA. A FPG test results between 110 and 125 mg/dl indicates pre-diabetes. A FPG of 126 mg/dl or higher indicates diabetes.
Type 1 diabetes occurs when the islet cells of the pancreas are destroyed and unable to produce insulin. Without insulin, the cells of the body are unable to allow glucose (sugar) to enter the cells of the body and fuel them. Without the hormone insulin, the body is unable to convert glucose into energy needed for activities of daily living. According to the ADA, 5-10% of Americans diagnosed with diabetes has type 1. It is usually diagnosed in children and young adults.
While type 1 diabetes is serious, each year more and more people are living long, healthy and happy lives. Some conditions associated with type 1 diabetes are: hyperglycemia, ketoacidosis and celiac disease. Some things you will have to know: information about different types of insulin, different types of blood glucose meters, different types of diagnostic tests, managing your blood glucose, regular eye examinations, and tests to monitor your kidney function, regular vascular and foot exams.
While symptoms may vary for each patient, people with type 1diabetes often have increased thirst and urination, constant hunger, weight loss and extreme tiredness.
Type 1 diabetes increases your risk for other serious problems. Some examples are: heart disease, blindness, nerve damage, amputations and kidney damage. The best way to minimize your risk of complications from type 1diabetes is to take good care of your body. Get regular checkups from your eye doctor for early vision problems, dentist, for early dental problems, podiatrist to prevent foot wounds and ulcers. Exercise regularly, keep your weight down. Do not smoke or drink excessively.
Type 2 is the most common type of diabetes as most Americans are diagnosed with type 2 diabetes. It occurs when the body fails to use insulin properly and eventually it fails to produce an adequate amount of insulin. When sugar, the primary source of energy in the body, is not able to be broken down and transported in the cells for energy, it builds up in the blood. There it can immediately starve cells of energy and cause weakness.
Also, over time it can damage eyes, kidneys, nerves or heart from abnormalities in cholesterol, blood pressure and an increase in clotting of blood vessels. Like type 1, even though the problems with type 2 are scary, most people with type 2 diabetes live long, healthy, and happy lives. While people of all ages and races can get diabetes, some groups are at higher risk for type 2. For example, African Americans, Latinos, Native Americans and Asian Americans/Pacific Islanders and the aged are at greater risk. Conditions and complications are the same as those for type 1 diabetes.
People with type 2 diabetes experience symptoms that are more vague and gradual in onset than with type 1 diabetes. Type 2 symptoms include feeling tired or ill, increased thirst and urination, weight loss, poor vision, frequent infections and slow wound healing.
Sources: NIH; American Diabetes Association; Harvard Health Publications
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
Preventing a fall can not only save your independence but also your life! Preventing injuries from falls reduces the need for nursing home placement. Injuries from falls are the seventh leading cause of death in people over the age of sixty-five.
The following suggestions will assist you in minimizing your risk of a fall:
Following these helpful hints will keep you safe by preventing a loss of balance and a potential fall!
Contributor: Janet M. Caputo, PT, DPT, OCS
Medical Reviewer: Mark Frattali, MD, ENT: Otolaryngology /Head Neck Surgery at Lehigh Valley Health Network
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles, visit our exercise forum!
