What medical problems do a carpenter, typist, truck driver, jackhammer operator, violinist, pianist and court stenographer have in common? Carpal tunnel syndrome! Over the past 10-15 years, carpal tunnel syndrome has moved to the forefront in medicine and has become water cooler conversation. So, what is carpal tunnel syndrome and how is it treated?
Carpal tunnel syndrome (CTS) is a nerve disorder caused by compression of the median nerve at the wrist. The median nerve is one of three main nerves that provide sensation to the hand. This nerve specifically supplies sensation to the thumb, index, middle, and half of the ring finger. In CTS, compression on the median nerve occurs as it travels through a narrow passage in the wrist called the carpal tunnel. The carpal tunnel is formed by eight bones in the wrist (the floor of the tunnel) and the transverse carpal ligament, a strong ligament traveling across the roof of the tunnel. Within the tunnel there are nine tendons, which are a bit smaller than a pencil. These tendons share this space with the median nerve. In the case where there is swelling on the structures in the carpal tunnel, a person can experience pins and needles, numbness, and aching in the hand.
To be properly diagnosed, a physician will discuss your symptoms and medical history and examine strength and sensation. A nerve conduction study, electromyography (EMG), and x-ray may be ordered to provide information regarding sensation in the median nerve distribution and confirm compression at the carpal tunnel.
Treatment focuses on the causes. Therefore, treatment suggestions may include activity modification and postural changes during activities. Other suggestions may include frequent rest periods, elevation, and exercises or stretching. Wrist splints are effective in relieving compression at the carpal tunnel and are typically recommended for night wear. Appropriate fit of the splint is vital. Occupational and physical therapists or certified hand therapists can check the fit of prefabricated splints or can fabricate a custom splint. The above-mentioned treatments all focus on decreasing inflammation and compression on the median nerve.
Your physician may order pain relievers or anti-inflammatory medication. A cortisone injection into the carpal tunnel may also be recommended to assist with decreasing inflammation near the carpal tunnel.
A referral to an occupational or physical therapist or certified hand therapist may be made. A therapist can provide information regarding the diagnosis, appropriate treatment, and symptom reduction. They can make recommendations to introduce into daily activities to allow appropriate positioning of the upper extremities. A therapist will also instruct individuals on helpful stretching exercises or fabricate a wrist splint. Other treatments include ultrasound, iontophoresis, and massage. The focus of therapy is to introduce changes and interventions that reduce inflammation at the carpal tunnel to assist with symptom relief.
Surgery, referred to as a carpal tunnel release, may be indicated if symptoms are significant and impair functional activity performance.
To reduce your chances of getting CTS:
Guest Contributor: Nancy Naughton, OTD, CHT, is a Doctor of Occupational Therapy and certified hand therapist, specializing in the rehabilitation of the hand and upper extremity at Hand Surgery Associates, Olyphant, PA.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

As most sports enthusiasts know, in 2021 Tiger Woods acquired an Achilles tendon rupture while training at home and in 2023 Aaron Rodgers, a former Green Bay Packer quarterback, did the same in the first game of the 2023/24 NFL season with the New York Jets. As with many sports injuries, it is painful and devastating and best managed by PREVENTION!
Spring is here! Many overjealous fitness enthusiasts will rush to pound the pavement and barely “fit in” a warm-up before participating. But, no matter how limited time is, skipping the warm-up is risky. This time of year, one can expect to feel a little cold and stiff, especially if you are over 40, and therefore a little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears. The Achilles tendon is one of the more common tendons torn. Prevention of muscle tears, including the Achilles tendon includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the Achilles tendon rupture and/or injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for complete Achilles tendon ruptures, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity and proprioceptive and agility drills are essential.
Eccentric Lowering and Lengthening: for the Achillies tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
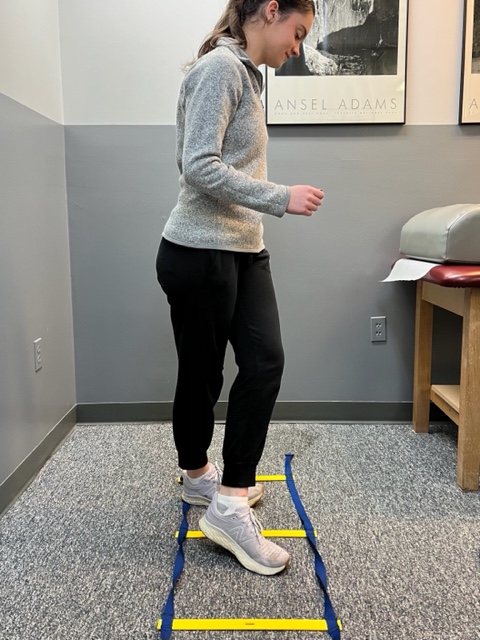
Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.
Sources: MayoClinic.com;Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from patients and sports fans about the nature of the Achilles Tendon rupture injury, recovery, and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to warm-up and exercise during the winter months. A little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears, especially Achilles Tendon rupture. The Achilles tendon is one of the more common tendons torn.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for tendons completely torn, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return to close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes: gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity – Photo 1) and proprioceptive and agility drills are essential (Photos 2 & 3).


In PHOTO 1a & 1b: Eccentric Lowering and Lengthening: for the Achillies tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
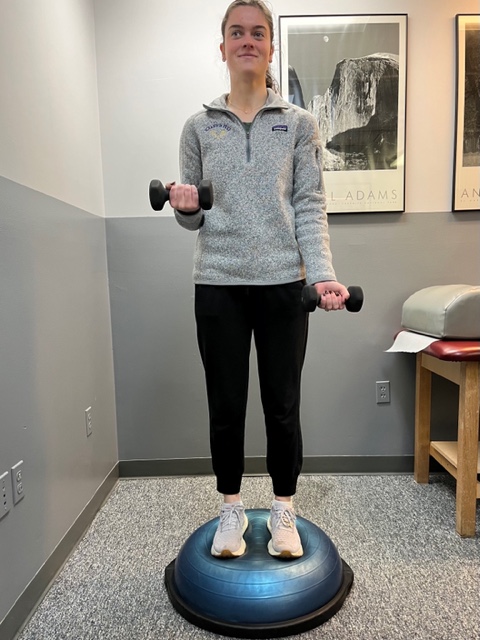
In PHOTO 2: Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
PHOTO 3: Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.
MODEL: Kerry McGrath, student physical therapy aide at Mackarey Physical Therapy
Sources: MayoClinic.com;Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
