At least once a week, a patient jokingly asks if they can get a “lube job” to loosen up their stiff knee joint. I respond by providing them with information about osteoarthritis and viscosupplementation, a conservative treatment administered by injection and approved by the FDA for the treatment of osteoarthritis of the knee.
Osteoarthritis (OA) is also known as degenerative arthritis. It is the most common form of arthritis in the knee. OA is usually a gradual, slow and progressive process of “wear and tear” to the cartilage in the knee joint which eventually wears down to the bony joint surface. It is most often found in middle-aged and older people and in weight bearing joints such as the hip, knee and ankle. Symptoms include: pain, swelling, stiffness, weakness and loss of function.
Your family physician will examine your knee to determine if you have arthritis. In more advanced cases you may be referred to an orthopedic surgeon or rheumatologist for further examination and treatment. It will then be determined if you are a candidate for viscosupplementation. While this procedure is the most commonly used in the knee, it has also been used for osteoarthritis in the hip, shoulder and ankle.
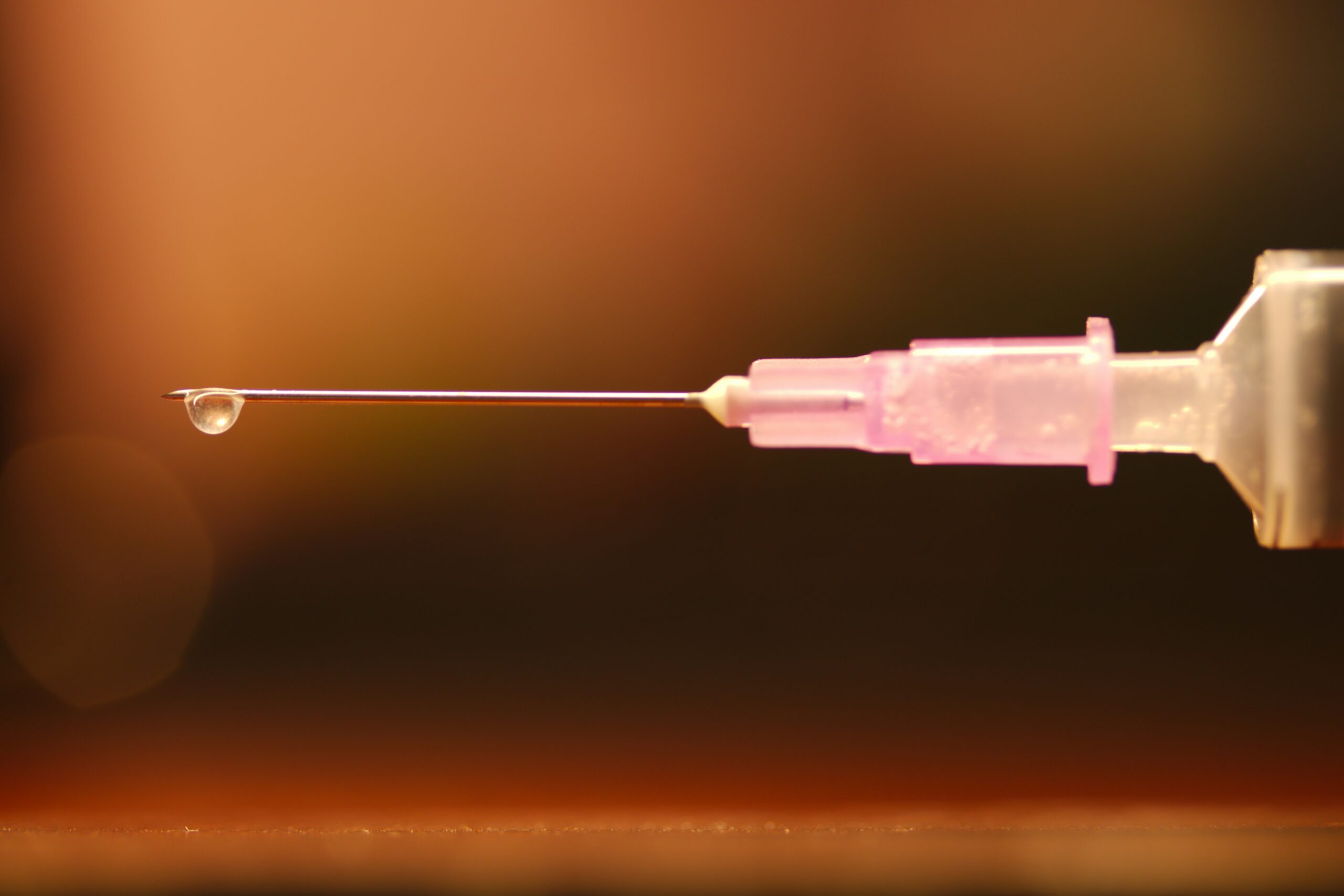
Viscosupplementation is a procedure, usually performed by an orthopedic surgeon or rheumatologist, in which medication injected into the knee joint acts like a lubricant.
The medication is hyaluronic acid is a natural substance that normally lubricates the knee. This natural lubricant allows the knee to move smoothly and absorbs shock. People with osteoarthritis have less hyaluronic acid in their knee joints. Injections of hyaluronic acid substances into the joint have been found to decrease pain, improve range of motion and function in people with osteoarthritis of the knee.
When conservative measures, such as anti-inflammatory drugs, physical therapy, steroid injections fail to provide long lasting relief, viscosupplementation may be a viable option. Often, physical therapy and exercise are more effective following this injection to provide additional long-term benefit. Unfortunately, if conservative measures, including viscosupplementation fails, surgery, including a joint replacement may be the next alternative.
In 1997 the FDA approved viscosupplementation for osteoarthritis of the knee. Presently, there are several products on the market. One type is a natural product made from the comb of a rooster. However, if you are allergic to eggs or poultry products or feathers, you should not use the natural product. The other medication is best used for patients with allergies because it is manufactured as a synthetic product.
The long-term effects of viscosupplementation is much greater when other conservative measures are employed:
SOURCES: Genzyme Co, Sanofi-Synthelabo Inc, Seikagaku Co. and American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Recently, a reader shared with me their concern about the aging process. They were not happy with the changes in their body, despite exercising regularly. New research suggests that there may be some forms of exercise that are better than others to counteract the aging process. With the accumulation of more and more birthdays, I too, am concerned about the changes in my body!
The deterioration and degeneration of the body associated with the aging process is well-documented and the musculoskeletal system is no exception. As we age, weight bearing joints of the lower body (hips and knees) frequently suffer from wear and tear degeneration. Loss of muscle mass and strength is also common with age. Specifically, damage to older muscles has been found to regenerate slowly and incompletely and the problem runs as deep as the cellular level as the mitochondria diminish in quality and quantity. However, there is good news: a recent study published this spring in Cell Metabolism suggests that certain types of exercise can actually regenerate and reverse the aging mitochondria.
As popular and common as exercise is, little is known about the influence and impact it has on the cellular level. A research team at the Mayo Clinic decided to answer this question and conducted an experiment to determine the cellular effects of different types of exercise on aging muscles.
The Mayo team chose 72 men and women and separated them into two groups: 30 and under and older than 64. All subjects were healthy but sedentary. Pretest analysis was performed for blood sugar levels, gene activity, muscle cell mitochondrial health, and aerobic fitness level. Subjects from the 30 and under group and the over 64 group were randomly assigned to one of four research groups.
Group One: Vigorous weight training 3-5 times per week, Group Two: Interval aerobic exercise on a stationary bike (pedaling hard and fast for four minutes followed by a recovery at a slow pace for three minutes then repeating the sequence 3 or more times) 3 times per week, Group Three: Moderate aerobic exercise on a stationary bike for 30 minutes 2-3 days per week and light weight lifting on the other 2-3 days, Group Four: Control group who did not exercise. After 12 weeks, lab tests were repeated and data compiled and analyzed.
In the 30 and under group as well as the over 64 group, all three experimental groups improved in fitness level and blood sugar regulation. As expected, Group One, the vigorous weight training group, showed the greatest gains in muscle mass and strength. Also, not surprisingly, Group Two, the interval training group, had the greatest gains in endurance. However, the most unexpected results came when retesting the muscle cells by biopsy. Only group two, the interval aerobic exercise group demonstrated the most significant improvement in the activity levels of their genes in both the young and older groups, when compared to the vigorous weight training and moderate exercise groups.
Moreover, the positive improvements in the genes of the older group far surpassed that found in the younger group. For example, in the younger group, 274 genes improved compared to 170 genes in the moderate exercise group and 74 in the vigorous weight training. In the older group, 400 genes were improved in the interval aerobic group while 33 for weight training and 19 for moderate exercise groups.
It is well known that loss of muscle mass and strength is common with age. Specifically, older muscles have been found to regenerate slowly and incompletely, and the problem runs as deep as the cellular level as the mitochondria diminishes in quality and quantity. However, this study suggests that interval aerobic exercise can regenerate and reverse the aging mitochondria. Healthier mitochondria can produce energy for muscle cells to function at a higher level.
Interval aerobic exercise can have anti-aging effects. In fact, the older your muscles, the more you will benefit from, not just moderate exercise, but more vigorous interval aerobic exercise. Furthermore, interval training may be applied, not only to aerobic exercise, but to weight training for the upper and lower body. According to the American College of Sports Medicine, high intensity interval training, also called HIIT workouts, involves a repetition of a series of high-intensity exercise (aerobic or weight training) for a specific period of time (3-5 minutes) followed by a specific period of rest or low-intensity exercise (1-3 minutes).
The intensity can be increased by speed or resistance. HIIT workouts have been associated with increased caloric expenditure with less exercise time, as well as improved strength and endurance. Most recently, it has been found to improve cell energy in the aging population. However, do not attempt to increase the intensity of your exercise program without consulting with your physician first. Once medially approved, consult with a Doctor of Physical Therapy to create a program specifically designed for you.
Therefore, if your gene pool is questionable like most of us, don’t use that as an excuse. There are things you can do to have a positive impact on your DNA to live longer and healthier…one of them is EXERCISE!
Visit your doctor regularly and listen to your body. Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

I think we would all agree, technology is a wonderful thing. However, like all good things, it comes at a price. Students and workers alike are suffering from the many physical effects of sitting for too many hours. Studies show the impact of prolonged sitting, especially with proper posture, are multifaceted: pain, headaches, vision problems, poor concentration, excess fat storage with weight gain. Studies strongly support the use of good posture, ergonomic workstations, posture stretches, frequent changes of positions, including the use of standing desks to prevent pain and injury. In fact, standing desks are not a new invention; they have been used by many to promote health and stimulate thought…Hemingway, Franklin and Jefferson all stood while they worked.
The average head weighs 10 to 12 pounds and when tilted down at a 45 degree angle the forces of gravity are multiplied by 5. While reading, studying or working on the computer with poor posture, one must support 50 or more pounds of pressure on the neck, middle and lower back for hours on end. It is no wonder why this activity is associated with headaches, neck and back pain, numbness and tingling in arms and legs, muscle spasms etc. Some studies report the lifetime prevalence of neck and shoulder pain in office workers as high as 80%.
Recent research has also correlated the amount of time an individual sits to a decrease in their average life expectancy. Seriously, watching television and sitting is literally killing us. The Heart and Diabetes Institute of Australia conducted extensive research on sedentary behavior, including a review of almost one million people. They used actuary science, adjusted for smoking, waist circumference, and diet and exercise habits to assess the specific effects that the hours of sitting in a day impacts a person’s life span. They found that sitting too long results in a decrease in muscle contraction of the big leg muscles and because these unused muscles need less fuel, more unused glucose (fuel) is stored in the muscle. High glucose levels result in high blood sugar, which leads to adult-onset diabetes and other health issues.
The deleterious effects of sitting in children have also come under scrutiny and it may impact the classroom. Due to technology, today’s classroom is more advanced in many ways. However, the traditional hard chair and desk remain unchanged. Not only are these, “one size fits all,” desks uncomfortable, current research suggests that they may also limit learning.
Recent studies show that standing desks promote not only a physically healthier child by expending more calories and lowering obesity but also improves focus and concentration to improve academic outcomes.
Research from Texas A&M Health Science Center found two landmark things about children who worked at standing desks such as Stand2LearnR, when compared to those seated: One, children burned more calories and obese children burned more than normal-weight peers. Two, children were more attentive in the classroom and engaged more with their teacher and their work when allowed to stand. Teachers in the study not only found the results to be favorable for fidgety, high-energy kids, but those who tend to be overweight and tired benefited greatly.
Researchers were quick to point out that there may be many ways to promote movement and limit sitting in the classroom that may also promote learning in a healthy way such as sitting on exercise balls or inflatable discs.
The average office worker sits for more than 10 hours per day between office work, sitting at lunch, checking email and social media at home. Amazingly, studies suggest that even vigorous exercise before and after work cannot overcome the damage from prolonged sitting. New products such as the “TrekDeskR,” allows a worker to work on a computer, phone, or do paperwork, while walking on a treadmill, has great health value. Also, other products such as VariDeskR, allows for frequent positional changes from sitting to standing while working. Even without using a standing desk, changing positions, such as standing during phone calls or meetings has proven to be valuable. Current Wisdom: Alternate standing (30-45 minutes) and sitting (15-30 minutes)
Spine problems can be prevented with good posture and proper body mechanics. Poor posture and improper body mechanics subject the spine to abnormal stresses that, over time, can lead to degeneration and pain. Good posture and proper body mechanics and frequent changes in positions, can minimize current spine pain and prevent recurrent episodes. Posture is the position in which you hold your body upright against gravity. Good posture involves positions that place the least amount of stress on the spine. Good posture maintains the spine in a “neutral” position. In a neutral spine, the three normal curves are preserved (a small hollow at the base of the neck, a small roundness at the midback and a small hollow in the low back). When viewed from the side, the upper back appears straight with a small hollow in the lower back.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Recently, a young woman came to my office with complaints of severe middle and lower back pain. On her first visit, I noticed her beautiful pink purse (big bag) and asked her permission to weigh the bag and discovered that it weighed 8 pounds. While 8 pounds does not seem excessive, the woman weighed 120 pounds and based on the research, would be advised to carry a 2.5-to-3.5-pound bag, (2-3% of her body weight).
A recent study shows that the average weight of a woman’s purse has increased by 38% and now exceeds 6 pounds. Despite technological advances, women have not found a way to simplify their lives, or at least what they think they need in their lives. High tech gadgets have only added weight to a purse already filled to the brim.
On a whim, I decided to ask permission to examine the contents of some of my patient’s purses. A typical purse includes the following: hairbrush, cosmetic bag, mirror, feminine products, keys, and sunglasses, reading glasses, checkbook, wallet, coupons, water bottle, and medications. Additionally, I discovered heavy high-tech products such as cellular phones, tablets, digital Bluetooth earpieces, and rechargers. Lastly, some women add the weight of a book or Kindle to the bag. Studies also show that the larger the bag and stronger the straps, the more items are stuffed in, resulting in a very heavy purse.
It is a pervasive attitude that a woman should never be stranded without her purse full of essentials. So, where is the problem? The problem is that carrying a heavy bag, usually on one side of the body, forces the body to tilt forward and to the opposite direction to compensate. Over time, this change in posture leads to neck, middle and lower back pain.
Consider the following suggestions to promote healthy use of a purse and prevent injury:
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Recently, two patients asked me when I thought it would be safe for them to return to their exercise programs after abdominal surgery. She stated that she was not sure how to properly and safely implement or return to her program.
This column will attempt to ensure a safe return to activity and exercise following general surgery such as gall bladder, appendix, hernia, etc. The post-operative patient has many questions: When is it safe to begin an exercise program? How do I begin? What is the best exercise? Which exercises are best? How do I know if the activity is too intense or not intense enough? Are there safe guidelines?
Before you begin, discuss your intention to exercise with your surgeon and primary care physician. Get medical clearance to make sure you can exercise safely. With the exception of short daily walks, don’t be disappointed if your surgeon requires you to wait at least until your 6 week post-op check-up to begin exercise.
While a 60 minute workout would be the long term goal, begin slowly at 15-20-30 minutes and add a few minutes each week. Make time to warm up and cool down.
Warm-up 5-10 minutes
Strength Training 10-15-20 minutes
Aerobic 10-15-20 minutes
Cool down 5-10 minutes
How to Monitor Your Exercise Program:
First, determine your resting heart rate by taking your HR (pulse) using your index finger on the thumb side of your wrist for 30 seconds and multiply it by two. 80 beats per minute is considered a normal HR but it varies. This is a good baseline to use as a goal to return to upon completion of your workout. For example, your HR may increase to 150 during exercise, but you want to return to your pre exercise HR (80) within 3-5 minutes after you complete the workout.
For those who are healthy, calculating your target heart rate (HR) is an easy and useful tool to monitor exercise intensity.
220 – Your Age = Maximum Heart Rate
EXAMPLE for a 45 year old: 220 – 45 = 175 beats per minute should not be exceeded during exercise.
For those concerned about calories expended during exercise.
NOTE: Keep the level at a light/moderate level for the first four to six weeks and advance to the moderate/heavy at week six. The Very Heavy Level may not be appropriate for 12 weeks post op is for those who have a reasonable fitness level and exercise 4-5 days per week.
Example of Data Found on Fitness Equipment
Remember, this is only accurate if you program your correct height, weight and age.
Level kCal/min MET
Light 2 - 4.9 1.6 – 3.9
Moderate 5 - 7.4 4 – 5.9
Heavy 7.5 - 9.9 6 - 7.9
Very Heavy 10 - 12.4 8 – 9.9
Always secure physician approval before engaging in an exercise program.
If the patient is on beta blockers (Atenolol, Bisoprolol, etc), it is important to use the Borg Rating of Perceived Exertion Scale (RPE) scale to determine safe exercise stress since exercise will not increase HR as expected:
0 - Nothing at all
1 - Very light
2 - Light
3 - Moderate
4 - Somewhat intense
5 - Intense (heavy)
6
7 - Very intense
8
9 - Very, very intense
10 - Maximum Intensity
NOTE: Keep the RPE at 2-3 the first 6 weeks post op and advance to level 3-4 at 8-12 weeks post op. Levels 5-6-7 are for those with a reasonable fitness level and exercise 4-5 days per week. The advanced levels should not be attained until 2-3 months of exercise and 3-4 months post op.
MEDICAL CONTRIBUTOR: Timothy Farrell, MD, is a general surgeon at GCMC.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Fall has arrived in NEPA and walking is a great way to enjoy the fall foliage. Moreover, a new study has found that walking can reduce lower back pain. Researchers in Australia followed more than 700 adults who had a recent onset of lower back pain (and were able to bear full weight without associated leg symptoms) and enrolled them in a walking program under the supervision of a physical therapist. One group walked for 30 minutes, 3-5 times per week and the control group remained inactive. Both groups were followed for more than three years and discovered that the inactive control group was twice as likely to suffer from repeated flare-ups of lower back pain when compared to the walking group.
It is good news for those who enjoy walking, however, for many who have not maintained an active lifestyle or have health issues, it is challenging to know where to begin. Also, beginning without a good plan can lead to injury and leave you discouraged. For example, those overweight and de-conditioned should not start a walking program too aggressively. Walking at a fast pace and long distance without gradually weaning yourself into it will most likely lead to problems.
There is probably nothing more natural to human beings than walking. Ever since Australopithecus, an early hominin (human ancestor) who evolved in Southern and Eastern Africa between 4 and 2 million years ago, our ancestors took their first steps as committed bipeds. With free hands, humans advanced in hunting, gathering, making tools etc. while modern man uses walking as, not only a form of locomotion, but also as a form of exercise and fitness. It is natural, easy and free...no equipment or fitness club membership required!
Walking to reduce or control lower back pain is only one of many important reasons to begin a program. According to the American Heart Association, walking as little as 30 minutes a day can provide the following benefits:
Anything is better than nothing! However, for most healthy adults, the Department of Health and Human Services recommends at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity, or an equivalent combination of moderate and vigorous aerobic activity. The guidelines suggest that you spread out this exercise during the course of a week. Also aim to do strength training exercises of all major muscle groups at least two times a week.
As a general goal, aim for at least 30 minutes of physical activity a day. If you can't set aside that much time, try several short sessions of activity throughout the day (3 ten or 2 fifteen-minute sessions). Even small amounts of physical activity are helpful, and accumulated activity throughout the day adds up to provide health benefit.
Remember it's OK to start slowly — especially if you haven't been exercising regularly. You might start with five minutes a day the first week, and then increase your time by five minutes each week until you reach at least 30 minutes.
For even more health benefits, aim for at least 60 minutes of physical activity most days of the week. Once you are ready for a challenge, add hills, increase speed and distance.
Keeping a record of how many steps you take, the distance you walk and how long it takes can help you see where you started from and serve as a source of inspiration. Record these numbers in a walking journal or log them in a spreadsheet or a physical activity app. Another option is to use an electronic device such as a smart watch, pedometer or fitness tracker to calculate steps and distance.
Make walking part of your daily routine. Pick a time that works best for you. Some prefer early morning, others lunchtime or after work. Enter it in your smart phone with a reminder and get to it!
Studies show that compliance with an exercise program is significantly improved when an exercise buddy is part of the equation. It is hard to let someone down or break plans when you commit to someone. Keep in mind that your exercise buddy can also include your dog!
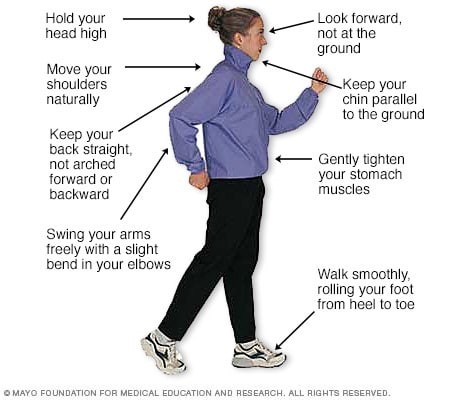
Like everything, there is a right way of doing something, even walking. For efficiency and safety, walking with proper stride is important. A fitness stride requires good posture and purposeful movements. Ideally, here's how you'll look when you're walking:
Sources : Sapiens.org; WebMD; Mayo Clinic, “Health & Science New”
Visit your doctor regularly and listen to your body
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Congratulations to more than 1,000 courageous runners who finished the 27th Annual Steamtown Marathon today. Most, if not all of you are waking up this morning with a little less jump in your step than you had yesterday.
As active people by nature, many of you will resist the logic of rest, despite the pain and stiffness in your muscles and joints. Therefore, I would like to offer some words of wisdom, based on science, to encourage you to adequately rest and allow your body to recover.
With adequate rest and recovery, an elite runner can quickly regain full form in 3-4 weeks, while an average runner may require 4-6 weeks. Meb Keflezighi, an elite American runner and winner of the 2014 Boston Marathon, is an excellent example of the merits of rest and recovery. However, he discovered it by accident…following the 2012 New York City Marathon, Meb developed a foot infection which required three weeks rest. With the Olympic Trials just 70 days away, Meb quickly regained his pre-injury fitness level to win the 2012 US Olympic Marathon Trials and join the US Olympic Team in London. It may be that his injury was fortuitous and allowed him adequate recovery time, (that he might not have otherwise allowed), preparing him for intensive training leading up to the trials.
The Effects of Running 26.2 Miles on the Body:
(RunNow.com - Jim Peskett)
One of the most obvious effects of running a marathon is significant muscle and joint pain and stiffness. It will set in after you sit for a while and attempt to get up and move around. For most, it will be more pronounced the day after the marathon, as you get out of bed and limp to the bathroom. Studies show that the leg muscles, (especially the calf muscles) display significant inflammation and necrosis (dead tissue) in the fibers of the muscle. In other words, the trauma to the muscles is so severe that tissue damage causes muscle cells to die. Consequently, studies found that muscle strength, power and endurance is compromised and required significant time to recover… sometimes as long as 4-6 weeks!
Additionally, many runners report severe bone and joint pain following the race. Some studies report findings of microfractures or bone bruising from the repeated and prolonged pounding of the marathon. It is purported that the stress on the joints may be related to: weight and body type, running shoes, running style and mechanics. While not dangerous, again, it is important to respect the stress placed on the body and allow adequate healing…LISTEN TO YOUR BODY!
Creatine kinase is an enzyme found in the brain, skeletal muscles and heart. It is found in elevated levels in the presence of cellular damage to these tissues, for example, following a heart attack. Similarly, significantly elevated creatine kinase levels are found in the blood of runners up to 4 days post marathon, demonstrating extensive tissue damage at the cellular level. It is important to note, that these enzyme markers are present, even if a runner does not experience muscle soreness. So, adequate rest for healing and recovery is required, regardless of soreness.
It is not a coincidence that the runners are more likely to contract colds and flu after intensive training or running 26.2 miles. The immune system is severely compromised after a marathon and without adequate recovery; a runner can become ill and ultimately lose more training time or will underperform.
FALSE: As stated above, enzyme levels that indicate cellular damage to the tissues are present in the post-marathon runner, even in those without significant pain.
FALSE: In addition to rest, drink, drink, drink - 24 ounces of water for every 2 pounds you lose after the marathon. This is based on pre and post exercise weight. You just burned 2,600 calories so avoid diet soft drinks. You need the glucose (sugar) boost. Also, don’t drink alcohol and use minimal amounts of caffeine (the equivalent of 1-2 cups of coffee). First, drink plenty of water and sports drinks (Gatorade) to prevent a diuretic like caffeine from messing up your fluid balance.
FALSE: Studies clearly show that the VO2 Max, (the best measurement of a runner’s endurance and fitness), is unchanged after one week of inactivity. And, after two weeks, the loss is less than 6% and can be regained quickly. Moreover, it is important to remember, without adequate rest and recovery, performance is comprised, not by the loss of VO2 Max, but by muscle-skeletal tissue damage, which renders the leg muscles of the runner weaker. Remember Meb Keflezighi!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

As summer fads and cool fall nights are upon us, many of us will prepare to put away some of our warm weather toys…closing the pool, storing kayaks and boats and packing up the “slip and slide.” However, one activity that can last well into the fresh breeze of fall is cycling. In fact, many feel that fall is the best time of year to jump on a bike and enjoy the ride! If you are looking for a kick start to riding your bike this fall, consider the 20th and final Tour de Scranton on Sunday, April 15, 2024. It is a fun-filled, noncompetitive bike ride through Scranton and neighboring communities. Tom and Betty Moreken, with the help of dedicated friends and countless supporters have raised over $400,000.00 to benefit addiction treatment and prevention in honor of their daughter Erin, a victim of drug addiction. I have had the privilege to know Tom and Betty and have always admired their resilience and selflessness to turn a negative into a positive and do something good for others. They and their friends truly represent everything that is good about the people of NEPA!
So dust off your bikes and join the fun at Tour de Scranton. Hopefully, it will entice you to ride the many beautiful and well-maintained trails that are available at the Countryside Conservancy and other locations in the Abingtons and the Lackawanna Heritage Valley Authority.
Tour de Scranton is the official “kick off” to biking season in NEPA. This year, on Sunday, September 15th, the 20th annual and final Tour de Scranton will offer a selection of several routes and distances for the novice and experienced rider at its non-competitive bike ride for riders of every age and skill level. This event supports “The Erin Jessica Moreken Drug & Alcohol Treatment Fund” which provides charitable gifts to qualified local organizations or individuals struggling with the disease of addiction. For more information visit: www.tourdescranton.com.
There are many obvious reasons to bike…cardiovascular fitness, burn calories, improve leg strength and others. But, the real question is, “what are the advantages of biking over other forms of exercise?” Glad you asked…
Prevention is the best management of musculoskeletal problems associated with biking. First, many of the problems associated with biking such as knee pain, buttock soreness, and tendonitis can be prevented through proper fitting. Furthermore, it is important that your equipment be in good working order such as tires, chain, brakes and pedals. Next, be sure to maintain a fairly good fitness level in order to bike safely. If you are a beginner, start slowly. Warm up and slowly bike for 10 to 15 minutes and build up over time. Practice the coordination of stopping, starting, shifting and braking. Work on good strength and flexibility of the hamstrings, quadriceps, calves and gluteal muscles. All of these muscles are necessary to generate pedal force. Balance is also important to safety and can be practiced on and off the bike. Be aware that adaptive equipment can modify your bike for added comfort and safety such as soft handlebar tape, seat post and front fork shock absorbers, padded biking shorts, c-out and gel pad saddle seats, and wider tires.
Be careful not to progress too quickly because inactivity to over activity in a short period of time can create problems. Overuse injuries such as tendonitis, can be avoided by cross training. Bike every other day and walk, run or swim on off days. Make sure to take time off to recover after a long ride. Use ice and massage to sore muscles and joints after riding.
Remember, cycling should be fun! Pain from improperly fitted and poorly maintained equipment is preventable. Excessive workouts and training rides should be kept to a minimum and consider cross-training in between.
EQUIPMENT: Helmets are a must! Also, keep your bike in good condition. Road bikes should have mirrors and reflectors. Use hand signals and obey traffic rules. Dress for weather and visibility. Have a first aid and tire patch kit, tire pump and tools. Seat comfort can be improved with gel cushion or split seat.
BE ALERT: for traffic, parked cars, pedestrians loose gravel and cracks in the road.
SOURCES: American Physical Therapy Association
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

“When is it safe for my child to start weight training?” This is a very common question asked by parents of young athletes who are looking for advice regarding their children’s participation in weight training. This month, for example, I received three such inquiries. While some who are eager to get a “competitive edge” may not be satisfied with the answer, these recommendations are grounded in the scientific literature and medical specialist with the hope to prevent injury and dispel fear and fallacy.
Weight training, weight lifting or resistive training all describes the use of a resistive force on a muscle to improve strength. While much attention has been given to the benefits of weight training in adults, much less has been written about its application in children.
According to the Journal of Pediatric Orthopedics, children less than 12 years old are considered prepubescent or before puberty. Teenagers who are between 12 and 19 are considered to be adolescents. Studies consistently demonstrate that strength gains are much more significant in adolescents than in preadolescents. It is important to note that these strength gains are not only from the enlargement of muscle fibers (hypertrophy), but also from the improvement in the coordination and efficiency in muscle contraction and the recruitment of motor units and fibers within the muscle.
Preadolescents lack the hormones necessary to develop masculine characteristics. Adolescents begin to produce the hormones of testosterone and androsterone to develop secondary sexual characteristics such as pubic hair and enlarged genitalia. In view of this, age 13-14 is the optimal age to safely begin and benefit from a well-designed weight training program.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

While many people celebrate the Labor Day holiday by firing up the grill, others will be shopping to get their students ready for the school year. One item on the shopping list should be a good quality and well-fitted backpack…to prevent lower back pain!
In 2018, the government of India announced a ban on homework and recently in Poland; the government ministers did the same. Can you imagine…a ban on homework? In an effort to promote student health and address recent surges in the incidence of back pain in the young, there will be no homework for students in grades one and two.
It was estimated that the majority of students ages 7 – 13 in India were carrying almost half their body weight. Not surprisingly, medical practitioners noticed a dramatic increase in reported cases of back pain among this group and decided to take action. In addition to the homework ban for grades one and two, Indian authorities have also implemented a limit of 10% of the student’s body weight.
Back pain in students seems to be universal. Each year, as students in the United States prepare to return to school from summer vacation, the subject of backpacks arises. The good news: when compared to purses, messenger bags, or shoulder bags, backpacks are the best option to prevent lower back pain. The bad news is, most of the 40 million students in the USA using backpacks, are doing so incorrectly.
Studies have found more than 33% of children had LBP that caused them to miss school, visit a doctor, or abstain from activity. Also, 55% of children surveyed carried backpacks heavier than the 10-15% of their body weight, which is the maximum weight recommended by experts. Additionally, the study noted that early onset of LBP leads to greater likelihood of recurrent or chronic problems. Backpacks that are too heavy are particularly harmful to the development of the musculoskeletal system of growing youngsters. It can lead to poor posture that may lead to chronic problems.
The following information on backpack safely is based, in part, by guidelines from The American Physical Therapy Association. Parents and teachers would be wise to observe the following warning signs of an overloaded and unsafe backpack:
Consider the following suggestions to promote backpack safely and prevent back injury:
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

