According to the United States Environmental Protection Agency, NEPA and all of Pennsylvania is experiencing a change in climate as indicated by a half a degree (F) in temperature, more frequent and heavy rainstorms and the tidal portion of the Delaware River is rising one inch every eight years. Last summer was one of our hottest on record and this summer more is expected. For those without air conditioning or access to a lake or pool, it will also be remembered as record setting warm temperatures. A local reader who cares for her elderly mother wrote to express her concern about dehydration in the elderly. Age, diet, illness and medications are some of the many reasons why elders suffer from dehydration not only in the summer heat, but year-round.
Next to oxygen, water is the nutrient most needed for life. A person can live without food for a month, but most can survive only three to four days without water. Even though proper hydration is essential for health, water gets overlooked as one of the six basic nutrients. Dehydration occurs when the amount of water taken into the body is less than the amount that is being lost. Dehydration can happen very rapidly (i.e. in less than eight hours). The consequences can be life threatening and the symptoms can be alarmingly swift.
In the body, water is needed to regulate body temperature, carry nutrients, remove toxins and waste materials, and provide the medium in which all cellular chemical reactions take place. Fluid balance is vital for body functions. A significant decrease in the total amount of body fluids leads to dehydration. Fluids can be lost through the urine, skin, or lungs. Along with fluids, essential electrolytes, such as sodium and potassium, are also perilously depleted in a dehydrated individual.
Dehydration is the most common fluid and electrolyte disorder of frail elders, both in long term care facilities and in the community! Elders aged 85 to 99 years are six times more likely to be hospitalized for dehydration than those aged 65 to 69 years. More than 18% of those hospitalized for dehydration will die within 30 days, and associated mortality increases with age. Men appear to dehydrate more often than women and dehydration is often masked by other conditions.
Elderly individuals are at heightened risk for dehydration for several reasons. Compared to younger individuals, their regulatory system (i.e. kidneys and hormones) does not work as well and their bodies have lower water contents. Older adults often have a depressed thirst drive due to a decrease in a particular hormone. They do not feel thirsty when they are dehydrated. This is especially true in hot, humid weather, when they have a fever, are taking medications, or have vomiting or diarrhea. They have decreased taste, smell, and appetite which contribute to the muted perception of thirst. Because of dementia, depression, visual deficits, or motor impairments, elderly people may have difficulty getting fluids for themselves. Many elderly individuals limit their fluid intake in the belief that they will prevent incontinence and decrease the number of trips to the bathroom. The medications that they are taking (e.g. diuretics, laxatives, hypnotics) contribute to dehydration.
Elders may suffer headaches, fainting, disorientation, nausea, seizure, a stroke, or a heart attack as a result of dehydration. The minimum daily requirement to avoid dehydration is between 1,500 (6.34 cups) and 2,000 ml of fluid intake per day. Six to eight good-sized glasses of water a day should provide this amount. Better hydration improves well-being and medications work more effectively when an individual is properly hydrated.
Those who care for the elderly whether at home or in a health care facility need to be alert to the following symptoms:
CHANGE IN MENTAL STATUS (CONFUSION)
WARM,MOIST SKIN WITH POOR SKIN ELASTICITY: gently pull the skin on the forehead and over the breastbone by pinching and releasing a skin fold; if the skin remains elevated for 3 seconds or more, dehydration is suspected
DRY, STICKY MOUTH WITH CRACKED LIPS AND DRY FURROWED TONGUE
DRYNESS IN NOSE
DECREASED BLOOD PRESSURE
INCREASED PULSE RATE (RACING HEART; HEART BEATING TOO QUICKLY)
CONSTIPATION
CONCENTRATED URINE WITH SCANTY OUTPUT: as the urine becomes more concentrated, it irritates the bladder and may increase the urge to void resulting in frequent, small voidings.
WEIGHT LOSS
SUNKEN, TEARLESS EYES
FAINTING WHEN STANDING UP (FEELING LIGHT-HEADED AND DIZZY WHEN STANDING AFTER SITTING OR LYING DOWN)
By the way, plain old tap water is a good way to replenish fluid loss. Keep in mind that some energy drinks not only have excess and unneeded calories but also contain sugar that slows down the rate at which water can be absorbed from the stomach. Consuming alcoholic and caffeinated beverages actually have an opposite, diuretic effect!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Part II of II
May is National Bike Month! For those who have a bike, now might be a good time to dust it off and enjoy the many beautiful and well-maintained trails that are available at the Countryside Conservancy at Lackawanna State Park, other locations in the Abingtons or the Lackawanna Heritage Valley Authority. For those who don’t have a bike, it might be a good time to get one!
However, whether you head out for 5 or 50 miles, ensuring a proper bike fit should be on your checklist. Riding a bicycle that is properly fit for your style and body will not only help to prevent injury but allow for a more comfortable riding experience. There are many things to take into consideration when checking your bike fit. First and foremost, you must choose a bike that fits your style of riding.
BIKE STYLES:
For the sake of simplicity 3 basic styles of bikes include Road bikes, Hybrid bikes and Mountain bikes. Road bikes are designed for long distance riders, hybrid bicycles can be used for longer distance riders, but usually accommodate a recreational cyclist, and mountain bikes are designed for dirt or gravel and technical trails. The next component of ensuring a proper bike fit is making sure that you have a good foundation by choosing the right sized frame. To find the right sized frame you can use the following guidelines as a way to start or simply ask the local bike shop or bike fit consultant of your choice for help.
Road bikes: When straddling the bike, you should have about 1” of clearance between your body and the top tube if the bike has a straight top tube (which runs parallel to the ground). When lifting the bike, you should have 1” clearance between the tires and the ground. If the bike has a sloping top tube (semi-compact design) you should have a clearance of 2” or more.
Mountain bikes: When straddling the bike lift the bike off the ground and you should have a minimum of 2” clearance between the ground and the tires. With full suspension bikes you will want 1”-2” standover clearance because when you sit on the bike the frame will become lower from compressing the suspension. More aggressive riders will likely have 3”-5” of clearance.
Comfort bikes: Standing over a comfort bike to choosing the right sized frame is not necessary. They are commonly designed with a steep sloping top tube and allow the rider to put feet firmly on the ground when the rider comes to a stop.
PROPER FIT:
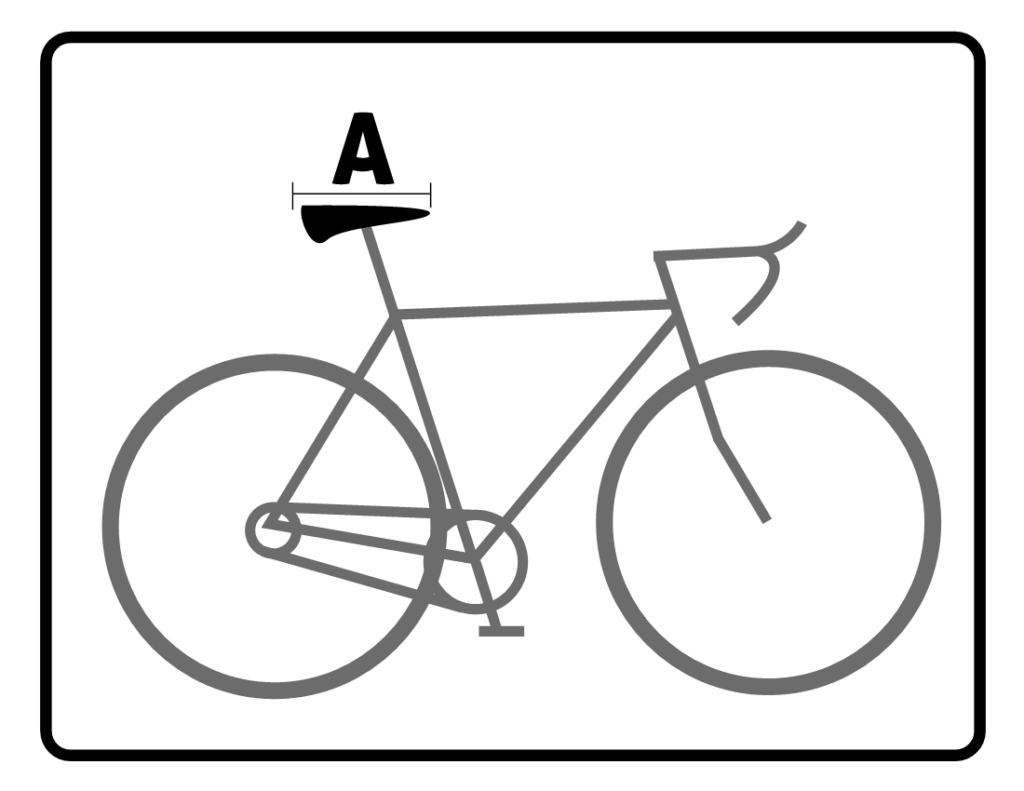
Now that you have right size for your bike you should adjust the components of the bike to allow for a more comfortable riding experience. Please use the diagram as a point of reference for the following tips. Also be sure to re-examine your bike fit after any bad falls. Keep in mind these measurements are meant to be used as a simple guideline and if you have any preexisting injuries or concerns please be sure to consult your local Physical Therapist or bike fit consultant.
Seat/Saddle:
Your Seat or saddle should be level (See “A” on diagram). If it is tilted too far forward there will be too much weight on hands, arms and lower back. If it is too far backward, there may be strain on LB and may lead to saddle related pain.
Your knee should be measured at the most extended position to adjust saddle height. (see “Knee to Pedal”)
The saddle should be a comfortable distance from handlebars. If it is too close it will place too much weight on your mid-back and arms. If it is too far it will put extra strain on your low back and neck. Also make sure seat is the proper width to ensure a more comfortable ride.
Handlebars (HB):
Your handlebar placement will affect your hands, shoulder, neck and back. The higher the handlebars are the more weight is placed on the saddle. Taller riders should have lower handlebars in relation to height of saddle
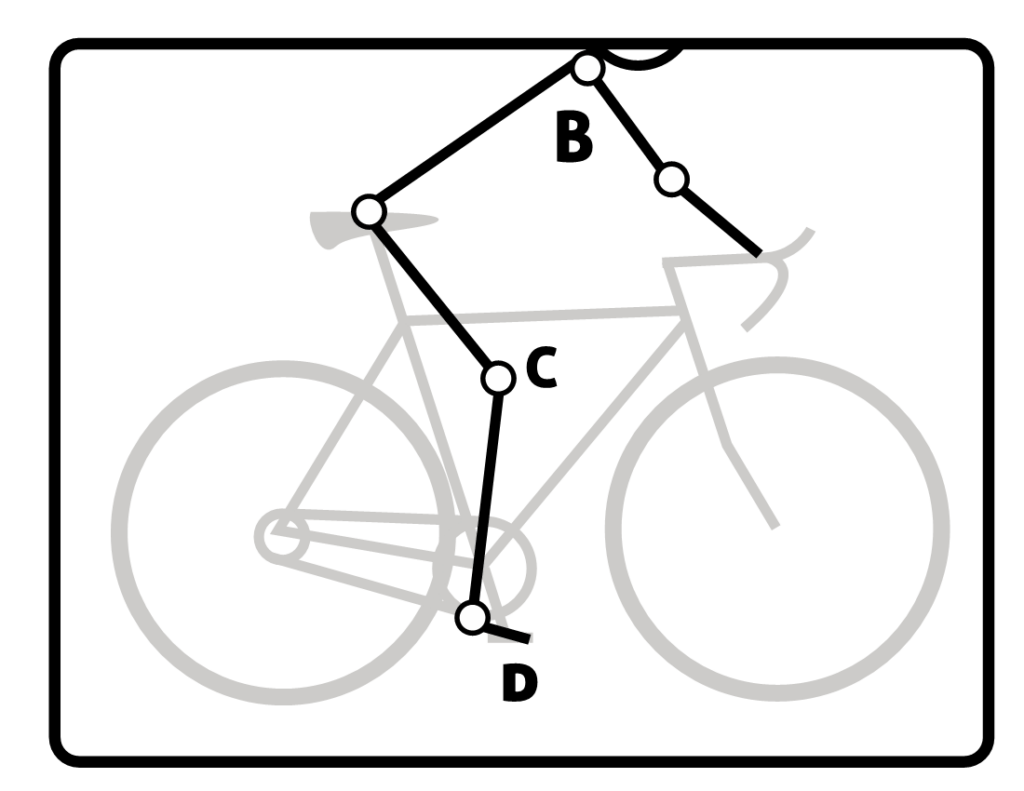
For road cyclists there should be a 90° angle between your arm (near the shoulder) and your trunk with a slight bend at your elbows of about 15° (See “B” on diagram).
Your trunk angle should be 25-35° if you are a road bike cyclist and 35-90° comfort/recreation cyclist
Knee to Pedal:
The knee to pedal measurement should be taken with the knee in the most extended position. There should be about a 25-35° angle at the knee (See “C” on diagram)
Foot to Pedal:
The ball of your foot should be over the pedal spindle (See “D” on diagram). This will allow for the best leverage, comfort and efficiency. Using a stiff soled shoe is recommended.
If you are a recreational cyclist, it’s a good idea to take all the proper steps in preventing injury. This article can be used as a reference point to help to prevent common cycling injuries, enhance your comfort and improve your riding efficiency. If you have any further questions about enhancing your bike fit, please contact your local physical therapist or bike fit consultant.
Sources: REI.com, APTA.org
Contributions & Illustrations: Sarah Singer, BFA, PTA
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Spring sports and outdoor activities are here…tennis, pickleball, baseball, soccer, running, walking, hiking, golfing, etc. One of the most common injuries associated with physical activity, especially after a sedentary winter or change in temperature is a “pulled hamstring.” This painful injury is not only for the weekend warrior. Well-trained, healthy and fit professional athletes often have their season interrupted for weeks and months due to a hamstring injury. What is the hamstring? How is it injured? What is the best treatment?
Hamstring Strain:
A hamstring strain is a tear of the muscle fibers of the muscle group in the back of the thigh called the hamstring. The hamstring muscle is a group of three muscles that run from the back of the hip (lower pelvis), crossing the back of the knee and attaches to the knee bone (tibia). The hamstring muscles work to extend the hip and bend the knee during running and walking activities. They are very active when an athlete changes direction, especially forwards and backwards or decelerating. This injury, like others muscle strains, varies in intensity.
Severe hamstring strain occurs when many muscle fibers are torn. The athlete may experience a sudden onset of severe pain in the back of the thigh and occasionally report a popping sensation. Pain, swelling and black and blue skin from tissue damage and bleeding is often reported. Also, pain is reproduced when attempting to bend the knee. In very severe cases, the boney attachment can be pulled so strongly that a small fracture can occur. Healing time can be as short as a few days or as long as weeks or even months.
The Most Common Causes of a Hamstring Strain:
Overuse – every time the knee is bent the hamstring muscles must contract. If there is not adequate time allowed for rest between workouts or competition, then the muscles may be fatigued and become vulnerable to injury. Also, overuse of the same muscles without rest may make them irritated and inflamed.
Inadequate Warm-up – a warm muscle stretches like a piece of gum warmed up in your mouth. When you pull the warm gum, it stretches. However, if you drink an ice cold drink with gum in your mouth and then stretch the gum, it will tear instead of stretch. A good warm-up will prevent tearing and prepare the nervous system for sudden movements and changes in direction.
Sudden Movement – quick sprint, sudden change in direction, quick turn with an unexpected force or slip.
Poor Body Mechanics – especially when moving or lifting a heavy load away from your center of gravity.
Forceful Contact or Loss of Traction – when a leg is forced away from the body by an outside force (tackle in football) or slip on grass or ice.
Diagnosis:
Your family physician will examine the back of your leg to determine if you have hamstring strain. Sometimes, pain in the buttocks and back of the leg can be referred from your lower back if the sciatic nerve is inflamed. In more advanced cases, you may be referred to an orthopedic surgeon for further examination and treatment. An X-ray, MRI or bone scan will show the extent of the tear and if the bone is involved. The diagnosis will determine if your problem is minor, moderate or severe.
Treatment:
There are many conservative options. Your family physician or orthopedic surgeon will help you decide which choices are best.
Anti-inflammatory Medications: such as aspirin, acetaminophen or ibuprofen to reduce pain and swelling.
Orthopedic Physical Therapy: such as heat, cold, ultrasound, electrical stimulation, joint mobilization, massage, range of motion exercises, strengthening exercises, and supportive compression strapping. Once pain free, a preventative training program is essential to prevent reinjury.
Activity Modifications: if it is not the week of the district tournament, rest, avoid running or stretching/stressing of the thigh muscles.
Supportive Devices: such as thigh wraps or sleeves, compression shorts (like those worn under basketball shorts) can provide compression and relief.
Prevention:
Recent studies have determined that a training program specifically designed to prevent hamstring injuries is effective, especially for the competitive athlete. This program includes:
High Intensity Training- regardless of the speed of your sport, high intensity, interval anaerobic training is critical. Interval sprints are the best example.
Simulate the Demands of the Sport – when training, simulate the specific demands of your sport… “train the way you play.” For example, in football, the average play lasts 7-10 seconds. Therefore, sprint on a count from the line of scrimmage for 7-10 seconds. First, sprint in a straight line. Then, sprint and cut at 3-5-10 yards. Then, sprint, cut and spin. Then, sprint figure 8’s.
Weight Train for Power and Strength/Weight Train for Speed and Endurance- traditionally, weight training is performed with high weights and low repetitions to increase power and strength and both arms or both legs are used at the same time. However, to prevent hamstring injuries, add a few sets of speed/coordination training by performing lifting with low weights and high reps. Also, alternate right and left legs to simulate normal walking speed.
Weight Training Using Negatives/Eccentrics – weight training with a concentration on lowering the weight against gravity, not raising it.
Exercise All Muscle Groups – of the lower body, not just the quads and hams. Include: Hip flexion, extension, abduction, adduction, internal & external rotation
Knee: flexion, extension
Ankle: flexion, extension, inversion, eversion
Warm -Up: a pregame slow jog or exercise bike and/or massage to the area to warm up the muscles prior to activity.
Stretching: Indian sit stretch, Hurdler stretch, Lying hamstring wall stretch
Strengthening Exercises: weight training for legs, including inside and back leg muscles, use weights or resistance tubing for leg curls and hip extensions.
Agility Drills: figure 8, cross-over, tire or disc running
Compression Shorts: like those worn under basketball shorts
Cool Down: use ice to the effected area after exercise or sport
SOURCES: Journal of Physical Medicine & Rehabilitation and American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
(and back, shoulders, etc)...
Germaphobes, cleaning zealots, neat freaks, and those with diagnosed or undiagnosed obsessive-compulsive disorder (OCD), this column is for you! If you would rather clean your bathroom floor than go for a walk on a beautiful sunny day, please read on. If you use a toothbrush on tile grout on a regular basis and take pride in the sparkle of your toilet bowl than beware… studies show that performing these tasks with too much vigor and passion might lead to back, neck, and shoulder and wrist pain.
For some, and you know who you are, (I am related to a few) spring cleaning can be a particularly exciting sporting event. It is almost an exorcism to rid a home of all its evil spirits, smudges, dust, dirt, germs, and odors. Every April curtains come off the windows to be washed and carpets rolled up, removed and cleaned. The surfaces under the curtains and carpets are sterilized with cleaning detergents, disinfectants and chemicals that would make sterile techniques in most hospital operating rooms seem inadequate. And that doesn’t include the heavy work: moving furniture, bedding, including mattresses and box springs.
As a physical therapist and survivor of childhood exposure to copious amounts of cleaning chemicals, I have come to learn that there are healthy and safe options for spring cleaning your home. Of course, the most obvious solution is to hire professional help if you can afford it. The other practical solutions are below:
10 Health Tips for Spring Cleaning:
Have a Plan - Take your time
It doesn’t have to be done in one day or one weekend!
Make a list, follow a schedule and do it over the course of 3-4 weeks
Do Not Move Heavy Furniture or Appliances by yourself
Get Help –
Use Sliders – to move heavy items like furniture
Be Cautious on Ladders and Stools
Falls are a leading cause of injury mortality in the US and 43% of fatal falls have involved a ladder, according to the Centers for Disease Control (CDC).
Avoid Reaching or stepping on the top step
Open and lock the ladder properly instead of leaning it against a wall
Use Proper Ergonomics
Lift Properly – back straight, knees bent
Incorrect Correct
Work at Eye Level – don’t work overhead for extended periods of time. Working overhead extends the neck and back and can lead to compression of the spine. This can cause pain, muscle spasms, headaches and pinched nerves which radiate symptoms into the arms and legs. Also, overextending and reaching with the shoulder, such as when cleaning windows, can lead to shoulder pain and stiffness from tendonitis or bursitis.
IncorrectCorrect
Wear a support if needed: knee or back brace, tennis elbow strap, arch supports
Avoid Prolonged Squatting – instead, kneel on a kneeling pad or wear knee pads
Use Caution Walking on Wet Surfaces
Use Caution Working Around Water and Electricity
Use Caution When Working with Household Cleaning Chemicals – provide adequate air circulation
Wear a Mask – when using cleaning chemicals or around dust, mold etc
Limit the Amount of Weight or Items You Carry – especially on the stairs
Take Breaks
Hydrate, Eat, and Rest
Stretch – neck, back, shoulders with a wall stretch
7 Safety Tips for Spring Cleaning:
Replace or Clean Filters for air and heat units
Clean out Medicine Cabinet
Get rid of unused and expired meds properly
Call your local pharmacist for details
Clean Attic, Garage, Cabinets and Basement of Dangerous Chemicals or toxic trash
Old paint cans, paint thinner, soiled rags, brushes etc
Contact your local government agency or recycling center for details
Remove mold and fungus from bathroom and laundry room
Replace Batteries in Smoke, Fire and Carbon Monoxide Detectors
Clean the Chimney – call a professional to protect you from carbon monoxide exposure
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
NEPA has had its share or snow this winter…and the recent storm added plenty of the pretty white stuff for work and play. Much has been written about the dangers of snow shoveling for your heart. However, while not fatal, low back pain is the most common injury sustained while shoveling snow. Heart attacks are also more common following wet and heavy snow.
Snow shoveling can place excessive stress on the structures of the spine. When overloaded and overstressed, these structures fail to support the spine properly. The lower back is at great risk of injury when bending forward, twisting, lifting a load, and lifting a load with a long lever. When all these factors are combined simultaneously, as in snow shoveling, the lower back is destined to fail. Low back pain from muscle strain or a herniated disc is very common following excessive snow shoveling.
Snow Shoveling as a Form of Exercise:
GOOD - For the Young and Healthy – studies show that snow shoveling for 15 minutes is considered moderate physical activity and extreme and vigorous physical activity when performed more than 15 minutes even for young healthy college students.
BAD – For the Older and Unfit – research clearly shows that there is a significant increase in heart attacks among snow shovelers. If you have any risk factors or medical condition and do not exercise regularly consult your physician.
Cold Weather – makes this activity even more difficult and physically stressful. Cold air makes breathing more labored and difficult and cold temps create added strain on the body.
People at High Risk of Illness Due to Snow Shoveling:
History of Heart Attack
History of Heart Disease
History of High Blood Pressure or High Cholesterol
Smokers
Inactive & Sedentary Lifestyle
Overweight
Elderly
10 TIPS FOR SAFE SNOW SHOVELING:
MEDICAL CLEARANCE: If you have any medical condition or risk factors consult your physician.
PAIN: Stop immediately if you experience any pain. Especially in the chest, left arm, jaw, face, neck, or lower back.
ERGONOMICS: Choose a snow shovel that is right for you:
An ergonomic shovel with a curved handle allows you to keep your back straighter or arched when shoveling
An ergonomic shovel with a shorter or adjustable handle length allows you to keep your back straighter and knees bent when shoveling. The right handle length allows you to arch your back 10 degrees with your knees slightly bent when the shovel is on the ground.A plastic shovel blade is lighter than a metal one and will be better for your spine.
A smaller blade is better than a larger blade. It may take longer but will stress your back less.
PUSH: When possible, push the snow. Do not lift it. Lifting is much more stressful on the spine. You can find shovels that are ergonomically designed just for pushing snow.
WARM – UP: Be sure your muscles are warm before you start to shovel. Cold and tight muscles are more likely to strain than warm, relaxed muscles. Layer and consider compression shirts or tights can help prevent cold and tight muscles.
LEVERAGE: When you grip your shovel, spread your hands at least 12 inches apart. This will improve your leverage and reduce strain on your lower back.
TECHNIQUE: Shoveling technique is very important. The American Academy of Orthopaedic Surgeons recommends:
Squat with your legs apart, knees bent and back straight.
Lift with your legs. Do not bend at the waist.
Scoop small amounts of snow into the shovel and walk when you want to dump it.
Do not hold the filled shovel with outstretched arms.
If snow is deep, remove in piecemeal, a few inches at a time.
Rest and repeat as necessary.
Move your feet and do not twist your back as you shovel or dump. Never throw snow over your shoulder
CAUTION: Be cautious shoveling wet snow. One full shovel can weigh 25 pounds.
Shovel wet snow slowly in piecemeal.
PACE YOURSELF: Take frequent breaks and stretch your back in the opposite direction of shoveling. For example: 1. Lean backwards and extend your lower back. 2. Pinch your shoulder blades together.
TECHNOLOGY:
Snow Blower - Use a self-propelled snow blower. It will put much less stress on your lower back than shoveling snow if used correctly. For example, push the blower with your legs and keep your back straight or arched and knees bent.
Ergonomic Shovels:
Rechargable Electric Snow Shovel: Toro, DeWalt, Voltask
2 Handle Shovels: ErgieShovel or Snow Joe ShovelutionPush Shovels: Garant Yukon or Garant Sleigh Shovel
WarmlyYours - HeatTrak® portable snowmelting system for roofs, gutters, driveways, sidewalks, stairs and handicapped ramps uses electric mats or runners for home or office which can be customized.
Sources: The Colorado Comprehensive Spine Institute; American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Part II of II
Patients often tell me that they would like to exercise but hesitate due to their knee or hip pain. They want to know what they should avoid, how to prevent and what is recommended to prevent or limit the progression of arthritis. Osteoarthritis (OA) is also known as degenerative arthritis. It is the most common form of arthritis in the knee. OA is usually a gradual, slow and progressive process of “wear and tear” to the cartilage in the joint which eventually wears down to the bony joint surface.
It is most often found in middle-aged and older people and in weight bearing joints such as the hip, knee and ankle. It causes gradual onset of pain, swelling and stiffness in the joint involved, especially after increased activity. While diet and exercise help, some people are more likely to develop OA based on previous trauma or injury, labor intensive occupations and genetics. Either way, we all get OA to some degree but there are a few things you can do to limit wear and tear to your joints.
However, OA is not an excuse to avoid exercise, but it is important to be smart about it. Regular exercise is essential to maintain a normal lifestyle for those with OA. However, if you make poor lifestyle choices, do the wrong exercise, use poor technique, or are too aggressive, you could flare-up your joints and do more harm than good.
Don’t Burn the Candle at Both Ends
Poor sleep can affect your joints. One study found that people with arthritis felt more pain after restless nights. One theory is that when you don’t sleep well, it triggers inflammation in your body, which may lead toOA over time.
Don’t Slouch and Slump
Posture matters. Sit up straight. When you slump in your chair, it puts more stress on your muscles and joints and tires them out. Two good posture stretches are making a double chin by bringing your head over your shoulders and the second is pinching your shoulder blades together.
Don’t Ignore Pain
The exercise mantra “no pain, no gain” may be appropriate for a young healthy athlete, however, it may prove counterproductive for most of us. It’s true that some muscle soreness is OK, but not if it lasts for days or if your muscles are swollen or too sore to move or to touch. Joint pain isn’t normal, so pay attention to it. If you think you overdid it, ease up on your exercises. If the pain won’t go away, check with your doctor.
Don’t Overdo Computer Time
It can literally be a pain in your neck -- and your elbows, wrists, back, and shoulders. The problem isn’t just bad posture, but that you hold it for too long. That overworks your muscles. It also puts pressure on the discs in your back. Set up an ergonomic workstation. If you’re in a soft chair, prop up your arms with cushions to take the load off your shoulders and your neck. Be sure to get up and move every hour.
Don’t Get Rigid and Repetitive in Your Exercise Routine
If you perform the same exercise, sport or activity every day, you use the same muscles and joints repeatedly. Remember, overtraining problems commonly occur in single sport athletes. Mix in fun sports and activities to break the monotony by adding fun activities such as golf, swimming, biking, skiing, hiking or playing tennis. Avoid weight bearing exercises two days in a row. Run one day, walk, swim or bike the next. Use the elliptical instead of the treadmill on various days. Limit intensity – only work out intensely 2-3 times out of 5 days per week.
Don’t Squat
Avoid squatting…deep squatting is bad for your hips and knees. Even when gardening, use a kneeling pad instead of bending down and squatting.
Don’t Smoke and Chew Tobacco
Nicotine from cigarettes and chewing tobacco cuts down on blood flow to your bones and to the cushioning discs in your back. It limits how much bone-building calcium your body can take in. It also breaks down estrogen, a hormone you need for bone health. And it slows new growth that thickens bones…which can lead to OA and osteoporosis.
SOURCES: WebMD, University of Pennsylvania
Visit your family doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Part I of II
Patients often tell me that they would like to exercise but hesitate due to their knee or hip pain. They want to know what they should avoid, how to prevent and what is recommended to prevent or limit the progression of arthritis. Osteoarthritis (OA) is also known as degenerative arthritis. It is the most common form of arthritis in the knee. OA is usually a gradual, slow and progressive process of “wear and tear” to the cartilage in the joint which eventually wears down to the bony joint surface.
It is most often found in middle-aged and older people and in weight bearing joints such as the hip, knee and ankle. It causes gradual onset of pain, swelling and stiffness in the involved joint, especially after increased activity. While diet and exercise help, some people are more likely to develop OA based on previous trauma or injury, labor intensive occupations and genetics. Either way, we all get OA to some degree but there are a few things you can do to limit wear and tear to your joints.
Your joints, which link your bones together, are sensitive to heavy loads. Every pound on your frame puts 4 pounds of stress on your knees. It also strains your back, hips, and feet.
That causes wear and tear that can lead to damage, aches, and pain. A poor diet, which can lead to being overweight, can also be the source of inflammation. That can make all your joints, including in your hands, stiff, painful, and swollen.
Don’t Text Too Much
“Texting thumb” is a real thing. Your tendons can get irritated and lock your thumb in a curled position. All that looking down at your phone is just as bad for your neck and shoulders, too. Every inch your head drops forward raises the load on your muscles.
Don’t Wear High Heels Too Often
While they might look styl”n, the higher the heel, the more your weight tips forward. Your leg muscles have to work harder to keep your balance and alignment, which can cause pain. When heels go up, so does the twisting force in your knees. If you wear them every day, you increase your odds of developing OA.
Don’t Wear the Wrong Shoes
Old, worn-out shoes will not adequately support your feet and ankles. That’ll throw your knees, hips, and back out of whack. Also, make sure your sneakers are right for your sport. High tops for basketball, for example, can protect your ankles from sprains and flip flops or summer beach shoes are not meant for long distances…especially if you are over 50.
Don’t Crack Your Knuckles
That satisfying pop comes from tiny bubbles bursting in the fluid around your joints, or from the ligaments snapping against the bone. While it might not cause OA directly, one study showed that this habit may cause your hands to swell and weaken your grip.
Don’t Carry a Heavy Bag
Whether it’s a purse, backpack, or messenger bag, packing too much can cause neck, back and shoulder pain. Heavy weight on one shoulder throws off your balance and your walk. If you tend to carry things only on one side, the constant pull overstretches your muscles and tires out your joints.
Don’t Use Wrong Muscles for the Job
When you put too much load on little muscles, your joints pay the price. If you need to open a heavy door, for example, push with your shoulder instead of your fingers. When you lift something off the floor, bend at your knees and push up with your strong leg muscles, instead of your arms.
Don’t Sleep on Your Stomach
While it might help with snoring, it may not be best for the rest of your body. Lying on your belly pushes your head back, which compresses your spine. Your head also will face in one direction for longer stretches than if you sleep on your back.
Don’t Skip Stretching
Gentle, comfortable, active stretching on a regular basis can help strengthen your muscles and tendons. It also can make them more flexible. That allows your joints to move more easily and helps the muscles around them work better.
Don’t Skip Strength Training
Once you turn 40, your bones start to get a little thinner and more likely to break. If you build muscle with strength training, it slows bone loss and triggers new growth. So, you not only get stronger muscles, but denser bones, too. Together, they stabilize your joints so you’re less likely to get hurt. In fact, studies show that the stronger your leg muscles, the less stress on your knees.
SOURCES: WebMD, University of Pennsylvania,
Visit your family doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
Next Week: Part II of II “Save Your Joints”
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Pediatricians and the American Academy of Pediatrics Recommend Parents Use Good Judgment
The American Academy of Pediatrics (AAP) cited studies suggesting that heavy use of electronic media may interfere with children’s speech and language development replace important playtime with parents and lead to obesity. Studies also have found that more than 90 percent of U.S. kids have used mobile devices and most started using them before age 1. The pediatricians’ group recommends no screen time for children up to age 2. Moreover, they recommend total screen time, including TV and computer; use should be less than one hour daily for ages 2 and older. Pediatricians don’t want parents to overreact. They understand that a little screen time on occasion is not likely to harm a child, especially if they are typically active and creative most of the day.
Dramatic increases in virtual education and toys powered by artificial intelligence (AI) make purchasing toys even more challenging. This may be the year to consider safe and appropriate gifts that promote physical activity. The academy’s website offers suggestions on ideal toys for young children, including balls, puzzles, coloring books and card games. Visit: AAP.org or HealthyChildren.org, the official parenting website of the AAP.
American Academy of Pediatricians Toy Recommendations:
Giving gifts to children is a favorite part of the holidays, whether they're wrapped under a tree or exchanged with the lighting of a candle. When choosing a toy for a child, the American Academy of Pediatrics recommends the toy be appropriate for the child's age and stage of development. This makes it more likely the toy will engage the child – and reduces the risk it could cause injury. Below are some additional tips from the AAP on toy selection and safety:
Appropriate: Select toys to suit the age, abilities, skills and interest level of the intended child. Toys that are too advanced will frustrate your child and may pose safety hazards for younger children.
Developmental: When choosing gifts for babies and toddlers, consider toys that will build developmental skills. Toys that can be manipulated, such as shape sorters, stacking blocks, and baby-safe puzzles, are great for developing fine motor, cognitive, and perceptual skills. For more tips on choosing toys for babies, visit HealthyChildren.org “toy selection.”
Purpose: If you are considering a digital device for a child or teen, such as a tablet, smart phone or game system, think about the purpose of the device and the rules you want to set around its use. For more information, see these tips on HealthyChildren.org “mindful technology use” and “digital media use for young children.”
Batteries/Magnets: Be cautious about toys containing button batteries or magnets. Children can have serious stomach, throat and intestinal problems – including death – after swallowing button batteries or magnets. In addition to toys, button batteries may be in musical greeting cards, remote controls, hearing aids, and other small electronics. Small, powerful magnets may be part of building toy sets. Keep button batteries and magnets away from young children and call your health care provider immediately if your child swallows one.
Electrical: To prevent burns and electrical shocks, do not give children under age 10 a toy that must be plugged into an electrical outlet. Instead, buy toys that are battery-operated.
Small Pieces: If you are buying a gift for a young child, look for toys without small pieces. Young children can choke on small parts contained in toys or games. Government regulations specify that toys for children under three cannot have parts less than 1 1/4 inches in diameter and 2 1/4 inches long. For more: HealthyChildren.org “how to buy safe toys.”
Balloons: Children can choke or suffocate on broken or uninflated balloons. Do not allow children under age 8 to play with them.
Ribbons/Strings: Remove tags, strings, and ribbons from toys before giving them to young children. Watch for pull toys with strings that are more than 12 inches long, because they could be a strangulation hazard for babies.
Read the Label: When your child receives a gift, be sure to read the label and instructions. Warning labels give important information about how to use a toy and what is the appropriate age. Be sure to show your child how to use the toy.
Storage: Parents should store toys in a designated location, such as on an open shelf or in a bin, and keep older kids' toys away from young children. If you use a toy box, choose one with no lid or a lightweight, non-locking lid and ventilation holes. Visit: HealthyChildren.org “toy box safety.”
Artificial Intelligence: Toys powered by AI chatbots which interact with children are often inappropriate. For example, these chatbots can talk in depth about sexually explicit topics and inform listeners where to find knives and matches.
SOURCE: American Academy of Pediatrics (AAP); healthychildren.org
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
More than 65 million people, almost 30% of the population in the United States, are actively involved in providing 20 or more hours of care for a chronically ill, disabled, or aged family member or friend each week. As our population continues to age, this number is expected to grow rapidly.
The role of a caregiver is multifaceted and often involves tasks and skills beyond the education or comfort level of most providers. Some examples include; managing money, paying bills, shopping, cleaning, maintaining and repairing a home, dispensing and injecting medications, cleaning wounds, changing dressings, catheter management, bed baths, assisting in position changes, transferring from the bed to the chair, ambulation, stair climbing, bathroom assistance for toileting and showering and many other responsibilities. Consequently, a caregiver is often at risk for mental, spiritual and physical fatigue or breakdown. It is no surprise that depression, illness and injury often plague a caregiver and eventually, the caregiver is in need of a caregiver. One of the most common injuries suffered by a caregiver is back pain.
Lower back pain (LBP) is one of the most common problems in our society. Over 90% of all Americans will suffer from it at least once in their lives. It is generally agreed that prevention is the best treatment for LBP.
TIPS FOR THE PREVENTION OF BACK PAIN FOR THE CAREGIVER:
Maintain Health & Fitness Level
As little as 10 extra pounds puts great stress on your lower back. It also makes it more difficult to maintain good posture. Eat well and exercise regularly.
Aerobic Exercise
Aerobic exercise will help prevent weight gain and stiffness for a healthier lower back. It will also help with the stress and depression associated with providing care for a loved one. Perform mild aerobic exercise such as walking 3-5 times per week for 30-45 minutes. You can also use an elliptical or bike at home while your loved one is resting. Get outdoors and take multiple short walks …go around the block a few times per day.
Core Exercises
Core stabilization exercises designed to strengthen the abdominal and lower back muscles will help prevent injury. Some examples of core exercises are:
Pelvic Tilt - lying on your back and performing a pelvic tilt as you flatten you lower back into the floor.
Pelvic Tilt and Heel Slide - lying on your back, hold a pelvic tilt as you slide your one heel up and down and repeat with the other heel.
Core on Ball - Perform arm exercises such as biceps and triceps with light weight while sitting on a therapeutic ball while simultaneously trying to hold an isometric contraction of your abdominal and lower back muscles.
Do Not Smoke
Smoking effects natural healing because it constricts the small blood vessels. Smokers have a much higher incidence of LBP and failure from lower back surgery.
Practice Good Posture & Body Mechanics
Good posture is critical for a healthy back. When sitting, standing or walking maintain a slight arch in your lower back, keep shoulders back, and head over your shoulders. In sitting, use a towel roll or small pillow in the small of the back.
Caregivers spend much of the day with their spine bent over a bed or chair feeding, bathing, and lifting a loved one. Postural exercises are designed to stretch your back in the opposite direction of this forward flexed position. Examples include:
Chin Tucks - tuck your chin back to bring head over shoulders.
Shoulder Blade Pinch - pinch your shoulder blades together.
Standing Arch - while standing put your hands behind back, extend lower back 10-20 degrees.
Perform slowly, hold for 3-5 seconds and repeat 6 times each 6 times per day.
Ergonomics
Sitting - When sitting, use an ergonomic work station and chair with a lumbar support and adjustable heights. Get close to your desk, keyboard and monitor.
Driving - If you drive long distances, use a lumbar support to keep an arch, sit close to your steering wheel to prevent bending forward.
Bending – Get an adjustable bed and raise it to a comfortable height when feeding, dressing or bathing your loved one.
Lifting - Think twice. First bend your knees and arch your back. Then, brace your abdominal muscles. Bend your spine forward as little as possible to lift the patient.
From Lying to Sitting in Bed - Bend your knees, maintain an arch in the back with head up, and bend over as little as possible. Bend the knees of your loved one; roll their trunk toward you to get their legs over the edge of the bed as you pivot their weight on their butt to get them sitting upright.
From Sitting in Bed to Sitting in Chair - Bend your knees, maintain an arch in the back with head up, and bend over as little as possible. Place your hands around the waist or on a transfer belt. Use your legs, turn with feet, and do not twist spine. Block the feet and knees of your loved-one with your feet and knees and use them to pivot and transfer from the bed to the chair. Be sure the chair is along side of the bed and arm of chair removed if possible before the lift.
Transfer Belt - Use a transfer belt around the waist of the patient. Grip the transfer belt, instead of the patient or clothing, during the lift or when ambulating.
Lower Back Lifting Belt - Also, if you have a back problem, consider using a lifting belt or back brace to protect your back when lifting the patient. Immediately following the lift, stand up straight and stretch lower back into extension.
Transfer belts and lower back lifting belts can be found online or at your local pharmacy.
Lift Chair – For patients that require maximum or moderate assistance and only one caregiver is available to lift or transfer, an electric lift chair should be considered.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Guest Author: Paul Mackarey, Jr. PT, DPT is clinic director and partner at Mackarey & Mackarey Physical Therapy Consultants, Scranton and Clarks Summit, PA.
The 2025 Pennsylvania rifle deer season begins November 30th and continues through December 13, 2025. Opening day is considered a holiday in the state of Pennsylvania as approximately 750,000 hunters from age 12 to seniors (including myself) will hike through the woods in search of a whitetail.
I am a whitetail, turkey, small game hunter, and an avid outdoors enthusiast with great passion for mountain biking, kayaking, hiking and mountain climbing in our state and national parks. After an extended period away from hunting (in the off season), I am eager to be back in the woods. When possible, I try to make time to shed hunt and scout in preparation for the upcoming season. While I am active during the summer, I am not necessarily in “hunting shape” and certainly not acclimated to cold, wet and windy conditions. I offer health and safety tips for hunters based on the knowledge of experts in the field and my expertise as a health care provider. Good luck and be safe!
Common Health Problems for Hunters:
Chest Pain/Shortness of Breath – overweight and deconditioned people must be very careful when overexerting themselves in the woods while hunting. This is especially true for those with a history of heart disease. Make sure you take your medication and drink plenty of fluids 24 hours before and while hunting. Eat a good breakfast with a balance of protein and carbohydrates. A bagel with peanut butter is a good quick start. Pack healthy snacks and water to sustain you.
Knee Pain- in the front of the knee or kneecap is common with hunting. This can happen from excessive hiking on uneven or hilly terrain in the woods, especially if there is weakness in the leg muscles. When walking downhill try this simple trick to keep your knees safe. Slightly bend at the knees and bring your buttock back so your knees stay over (or slightly behind) your toes to reduce stress on the joint.
Neck, Lower or Middle Back Pain- can be caused by prolonged hiking with a heavy load or prolonged sitting in a tree stand in slouched positions, especially if one has tight hamstrings. Field dressing and carrying the deer out of the woods is also very stressful on the back. Take multiple breaks and stretch backwards, (the opposite direction of bending over to drag the deer). Also, consider where you want to position your hunt, avoid large hills that you may have to drag the deer up on the way out.
Shoulder Pain- can occur from recoil of a gun shot or the overhead activity of climbing a tree.
Hamstring Pain- can occur if the muscle is tight or weak. Prolonged walking, bending over and large steps over fallen trees can contribute to this problem. When free walking in the woods, look for the path of least resistance.
Ilio-Tibial Band Pain- when walking on the side of a hill there is a difference in the length of the legs. Overtime, this can lead to pain on the outside of the hip and leg.
Foot Numbness or Pain- can occur from prolonged squatting or poor fitting shoes/boots. However, lower back pain can also be associated with these symptoms.
Hand Numbness or Pain- can be caused by repeated recoil of the gun on the shoulder. Also, this may be associated with prolonged pressure of a shoulder strap or leaning on something under the arm.
Preparing Your Body for Hunting:
Prevention is the best management of most musculoskeletal and safety problems associated with hunting. First, one can prevent many of the above problems through proper fitting of equipment, clothing and shoes/boots.
Fitness - Be sure to maintain a fairly good fitness level in order to hunt safely. Begin an exercise and walking program 2-3 months before hunting season. If you are a beginner, start slowly. Warm up and slowly walk for 10 to 15 minutes and build up over time. Slowly add hills to your walking program.
Clothing - Wear your hunting clothing, such as boots to break them in while walking for exercise. Drytech clothing instead of cotton can keep you warm and wick moisture away from the body.
Move & Stretch - As hunters, we sit in our stand or blind and stay still for long periods of time in cold temperatures. This results in a cold and stiff body. When leaving your setup, give your body time to wake up before you start hiking out. Bend the knees or perform small squats repeatedly to get blood and warmth back into the legs. Stretch your spine backwards (the opposite of sitting) to prepare your spine for your heavy pack and do some heel raises for the ankles.
Strength Exercises - Work on the strength and flexibility of the quadriceps, calf and gluteal muscles. Instead of using the elevator, climb stairs throughout the day to work these muscles. Be careful not to progress too quickly because a drastic change from inactivity to over activity in a short period of time can create problems.
Be Aware - Know your limitations and adapt to them. Injuries most commonly occur when we overestimate what our body can do or choose to push through pain. Listen to your body, if you have pain, stop and modify your activity. In addition, scout areas that are more easily accessibly in the woods that will still attract deer. This will lead to less stress on your body and when successful, you have an easier drag!
Use technology to your advantage. Using hunting apps and maps such as HuntWise, OnX or HuntStand, can help give you an idea of the terrain you will be exposed to prior to entering the woods. It will be easier to map out a less strenuous approach into the woods and minimize the load you place on your body.
Remember, hunting should be fun! Pain from poorly fitted and improperly maintained equipment and clothing can be avoided with good planning. Moreover, injury and death from inactivity and poor fitness is also preventable.
Visit your doctor regularly and listen to your body. Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!




 Incorrect
Incorrect  Correct
Correct Incorrect
Incorrect  Correct
Correct










