Last week’s column was dedicated to Rosie Malloy as we discussed the importance of laughter for health and wellness. In this column, I will discuss one of the most understated benefits of exercise – mental health! Specifically, aerobic exercise (exercise that increases your heart rate for 30 minutes or more) such as walking, biking, running, swimming, hiking, elliptical & stepper machines to name a few, is the secret to “runner’s high.” This exercise euphoria is not limited to runners alone, but all who engage in aerobic exercise are more likely to experience high energy, positive attitude, and mental wellness by helping reduce depression.
Physical activity, specifically aerobic exercise, is a scientifically proven useful tool for preventing and easing depression symptoms. Studies in the British Journal of Medicine and the Journal of Exercise and Sports Science found that depression scores were significantly reduced in groups that engaged in aerobic running, jogging or walking programs, 30-45 minutes 3-5 days per week for 10-12 weeks, when compared to a control group and a psychotherapy counseling group.
Depression is the most common mental disorder and is twice as common among women as in men. Symptoms include: fatigue, sleeplessness, decreased appetite, decreased sexual interest, weight change, and constipation. Many of these symptoms are likely to bring an individual to their family physician. Unfortunately, depression is on the increase in the United States. According to the National Ambulatory Medical Care Survey, in the 1990’s, 7 million visits to a primary care physician were for the treatment of depression. 10 years later the number doubled.
According to copious amounts of scientific research, exercise improves health and wellness and reduces depression in two ways, psychologically (mentally) and physiological (physically).
SOURCES: British Journal of Medicine: Journal of Exercise and Sports Science

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.comPaul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

I am sure that many of you feel as I do…it is hard to believe that I am living in the year 2025! Moreover, I hope you share my sentiments that each year, despite the trials and challenges of each month, week, day, and minute, is a gift, not to be taken for granted and 2025 is no different. And that is why we resolve at this time each year to make a concerted effort to improve ourselves; mentally, physically and spiritually, so that we may live a longer and healthier life, to spend more time with the friends and family we love.
Not surprisingly, getting physically fit and losing weight are the top resolutions to begin each New Year, even 2025. According to the University of Pittsburgh Medical Center, 10 million Americans choose to join one of the 45,000 health clubs and hope to get fit and healthy for life. Unfortunately, if starting an exercise program is the hard part, than sticking to it is the hardest part.
Once the initial excitement and enthusiasm wears off after the 2025 new year, so does the discipline and determination necessary to overcome the many distractions in our lives to make exercise a priority for life. Diane Klein, PhD polled long-term exercisers (those exercising at least 3 times per week for more than 13 years) what motivated them to “stick with the program.” The answers are in order of importance. Please note that “appearance” was NOT at the top of the list.
Source: WebMD, Mayo Clinic
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

While I normally do not address the topic of shoveling snow until January, considering recent weather events, I thought it might be valuable to present it sooner. Much has been written about the dangers of snow shoveling for your heart. However, while not fatal, low back pain is the most common injury sustained while shoveling snow. Heart attacks are also more common following wet and heavy snow.
Snow shoveling can place excessive stress on the structures of the spine. When overloaded and overstressed, these structures fail to support the spine properly. The lower back is at great risk of injury when bending forward, twisting, lifting a load, and lifting a load with a long lever. When all these factors are combined simultaneously, as in snow shoveling, the lower back is destined to fail. Low back pain from muscle strain or a herniated disc is very common following excessive snow shoveling.
Sources: The Colorado Comprehensive Spine Institute; American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Recently, two patients asked me when I thought it would be safe for them to return to their exercise programs after abdominal surgery. She stated that she was not sure how to properly and safely implement or return to her program.
This column will attempt to ensure a safe return to activity and exercise following general surgery such as gall bladder, appendix, hernia, etc. The post-operative patient has many questions: When is it safe to begin an exercise program? How do I begin? What is the best exercise? Which exercises are best? How do I know if the activity is too intense or not intense enough? Are there safe guidelines?
Before you begin, discuss your intention to exercise with your surgeon and primary care physician. Get medical clearance to make sure you can exercise safely. With the exception of short daily walks, don’t be disappointed if your surgeon requires you to wait at least until your 6 week post-op check-up to begin exercise.
While a 60 minute workout would be the long term goal, begin slowly at 15-20-30 minutes and add a few minutes each week. Make time to warm up and cool down.
Warm-up 5-10 minutes
Strength Training 10-15-20 minutes
Aerobic 10-15-20 minutes
Cool down 5-10 minutes
How to Monitor Your Exercise Program:
First, determine your resting heart rate by taking your HR (pulse) using your index finger on the thumb side of your wrist for 30 seconds and multiply it by two. 80 beats per minute is considered a normal HR but it varies. This is a good baseline to use as a goal to return to upon completion of your workout. For example, your HR may increase to 150 during exercise, but you want to return to your pre exercise HR (80) within 3-5 minutes after you complete the workout.
For those who are healthy, calculating your target heart rate (HR) is an easy and useful tool to monitor exercise intensity.
220 – Your Age = Maximum Heart Rate
EXAMPLE for a 45 year old: 220 – 45 = 175 beats per minute should not be exceeded during exercise.
For those concerned about calories expended during exercise.
NOTE: Keep the level at a light/moderate level for the first four to six weeks and advance to the moderate/heavy at week six. The Very Heavy Level may not be appropriate for 12 weeks post op is for those who have a reasonable fitness level and exercise 4-5 days per week.
Example of Data Found on Fitness Equipment
Remember, this is only accurate if you program your correct height, weight and age.
Level kCal/min MET
Light 2 - 4.9 1.6 – 3.9
Moderate 5 - 7.4 4 – 5.9
Heavy 7.5 - 9.9 6 - 7.9
Very Heavy 10 - 12.4 8 – 9.9
Always secure physician approval before engaging in an exercise program.
If the patient is on beta blockers (Atenolol, Bisoprolol, etc), it is important to use the Borg Rating of Perceived Exertion Scale (RPE) scale to determine safe exercise stress since exercise will not increase HR as expected:
0 - Nothing at all
1 - Very light
2 - Light
3 - Moderate
4 - Somewhat intense
5 - Intense (heavy)
6
7 - Very intense
8
9 - Very, very intense
10 - Maximum Intensity
NOTE: Keep the RPE at 2-3 the first 6 weeks post op and advance to level 3-4 at 8-12 weeks post op. Levels 5-6-7 are for those with a reasonable fitness level and exercise 4-5 days per week. The advanced levels should not be attained until 2-3 months of exercise and 3-4 months post op.
MEDICAL CONTRIBUTOR: Timothy Farrell, MD, is a general surgeon at GCMC.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from patients and sports fans about the nature of the Achilles Tendon rupture injury, recovery, and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to warm-up and exercise during the winter months. A little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears, especially Achilles Tendon rupture. The Achilles tendon is one of the more common tendons torn.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for tendons completely torn, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return to close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
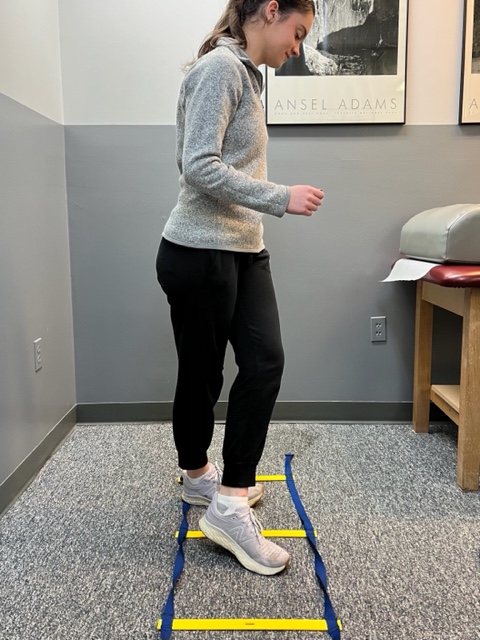
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes: gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity – Photo 1) and proprioceptive and agility drills are essential (Photos 2 & 3).


In PHOTO 1a & 1b: Eccentric Lowering and Lengthening: for the Achillies tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
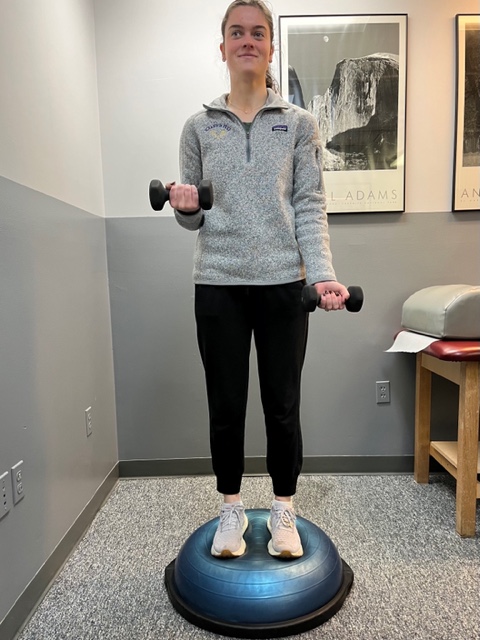
In PHOTO 2: Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
PHOTO 3: Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.
MODEL: Kerry McGrath, student physical therapy aide at Mackarey Physical Therapy
Sources: MayoClinic.com;Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
