This year, Valentine’s Day is Valentine’s Weekend! And, while you may wonder what that has to do with health and wellness, you might be surprised to learn that love can be good for your health! Studies show that it is in our DNA to seek out good relationships and that these solid relationships can lead to a happier, safer and healthier life. Conversely, infatuation and less committed, volatile relationships that are “on and off,” are very stressful and unhealthy. But those fortunate to participate in a stable and satisfying long-term relationship are the beneficiaries of many health benefits! Whether you have spouse, partner, or close friend, (love is love is love), feeling connected, respected, valued, and loved is critically important to your health and wellness!
SOURCES: WebMD

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

I wish I could tell you that after turning 50, there are health issues associated with age I plan to be mindful of and address proactively. Unfortunately, that ship has sailed for me well more than a decade ago. So, I share this medical information, not only as a health professional but also as an experienced senior.
Entering the fifth decade is not all dome and gloom. Often, this decade is associated with an established family, gratifying career, good health and acquired self-confidence…realizing that life does not have to be perfect to be wonderful!
However, research tells us that as the body ages, even small changes at the cellular level can be manifested into big changes and problems over time. Nine of ten older adults have some type of chronic disease and eight of ten have more than one. But the good news is that, with a modicum of effort, most of these illnesses can be controlled or prevented, including regular doctor visits, health screening and testing, and lifestyle changes.
While it is normal to experience some weight gain is expected with age. However, uncontrolled, the average person will gain 1-2 pounds per year, leading to 11 pounds per decade, according to the National Institutes of Health. Consequently, almost 45% of Americans between 40 to 60 are obese. Obesity is associated with at least 20 chronic illnesses such as high blood pressure, heart disease, diabetes, cancer, and arthritis.
SCREEN: Body Mass Index (BMI)
TREATMENT: Diet, Exercise, Lifestyle, Medications, Surgery
With age, the flexibility of blood vessels loses elasticity and, unchecked, two out of three adults over 60 have high blood pressure. While genetics is a factor, there are a few things that you can control such as diet (salt, calories), exercise, weight, stress, and smoking.
SCREEN: Blood Pressure Test, Lab Tests, Electrocardiogram (ECG/EKG)
TREATMENT: Diet, Exercise, Lifestyle, Medications
Plaque buildup in the arteries of the heart begins in childhood and advances rapidly with age. 6-7 percent of US adults between the ages of 40 and 60. 20% of men and almost 10% of women between the ages of 60 and 80 have heart disease.
SCREEN: Blood Pressure, Cholesterol testing, Blood Sugar Testing, Imaging (ECG/MRI)
TREATMENT: Diet, Exercise, Lifestyle, Medications, Surgery
10 % of Americans have diabetes and the percent only increases with age. Diabetes is associated with many serious chronic illnesses such as heart disease, blindness, kidney disease and others.
SCREEN: Blood Test for blood sugar levels such as A1C, fasting plasma glucose test and random plasma glucose test
TREATMENT: Diet, Exercise, Lifestyle, Medications
In many cases osteoarthritis (wear and tear of joints) is often associated with age. However, lifestyle, joint injuries, inactivity, obesity and diabetes play a significant role.
SCREEN: Physical Exam, Functional Scores, Xrays, MRI, CT, US
TREATMENT: Diet, Exercise, Physical Therapy, Lifestyle, Medications (NSAID’s, Steroids, Viscosupplementation), Bracing, Surgery
Loss of bone density and strength is associated with age and certain metabolic conditions such as early menopause, thyroid disease, prolonged use of blood thinners and steroids. However, a diet rich in vitamin D, regular weight bearing exercises such as walking, jogging, dancing etc can go a long way.
SCREEN: Fracture Risk Assessment Tool (FRAX), Dual-Energy X-Ray Absorptiometry (DEXA) TREATMENT: Diet, Exercise, Physical Therapy, Lifestyle, Medications (Oral and Injection)
Losing balance with age is a common problem due to changes in the vestibular system (balance system in the brain), loss of muscle strength and joint flexibility, and compromised vision and hearing. This can often lead to falls, head injuries and fractures.
SCREEN: Timed Up and Go (TUG) Test, Morse Fall Scale
TREATMENT: Physical Therapy – Falls Prevention Program/Balance Training , Diet, Exercise, Lifestyle, Environmental Modification, Vision/Hearing Testing
Almost 10% of adults between the ages of 55 and 65 have some form of vision and/or hearing loss. This can lead to many problems such as balance and falls as well as isolation and depression.
SCREEN: Regular Hearing Tests/Vision Testing
TREATMENT: Corrective Devices
Both men and women suffer from bladder problems with age... especially frequency and control. It can impact lifestyles in many ways. Often adults fail to hydrate properly, especially when traveling, to control urgency. This can lead to other health problems.
SCREEN: Urine Analysis, PSA, Imaging, CT Urogram, Urine Cystoscopy, Ultrasound,
TREATMENT: Diet, Exercise, Lifestyle, Avoid Caffeine and heavy lifting, Medications, Surgery
As the body ages, so too do the cells that make it up. Often these cells change into cancer different parts of the body. Skin, colon, breast, prostate, lung, throat, etc. Today, however, much progress has been made for early detection and treatment.
SCREEN: Physical Exam (Skin Exams), Lab Tests (blood work, PSA), Imaging (CT, Mammography, MRI), Genetic Testing, Pap Smears, HPV Tests, Colonoscopies/Stool Tests, Multi-Cancer Early Detection (MCED)
TREATMENT: Diet, Exercise, Physical Therapy, Lifestyle, Medications, Chemotherapy, Radiation, Immunotherapy and Targeted Therapy Surgery specific to the cancer type.
Age related mental health issues are vastly unreported and diagnosed. Medical problems can contribute to mental health such as high blood sugar levels and some infections. Overall, lifestyle, environmental factors and family structure and support are particularly important.
SCREEN: No Single Test – Combination of Tools including - Neurological and Cognitive Tests, Brain Scans (CT/MRI), Blood tests, Genetic Testing
TREATMENT: Diet, Exercise, Physical Therapy, Lifestyle, (avoid excessive toxins like alcohol and nicotine), Medications, Environmental Modifications.
SOURCES: WebMD, NIH, Mayo Clinic, Alzheimer’s Association, American Cancer Society, American Heart Association, American Diabetes Association
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Age-related changes to your body are normal and expected. For example, loss of muscle tone, stiffness in joints, and loss of balance. With effort, some of these changes can be retarded and managed with stretching, strengthening and balance exercises. The brain is no different…it can slow down and lead to memory lapses. However, for most of us, it too can be managed and with a little effort, be kept sharp and clear.
Many experts feel that exercise is the best method to maintain not only physical health but mental health. Regular exercise can prevent the things that contribute to memory loss with age such as; diabetes, high blood pressure, high cholesterol, obesity and stroke.
Specifically, aerobic exercise may be most beneficial. Aerobic exercise is any type of sustained exercise that strengthens the heart and lungs to improve the body’s use of oxygen. This may include running/jogging, brisk walking, cycling, swimming, rowing, and the use of a treadmill, elliptical, stepper or similar device, at light to moderate intensity which requires the use of oxygen to adequately meet the oxygen demands of the body for an extended period of time. The generally accepted time and frequency is at least 30 minute sessions performed three or more times per week. Two 15 minute or three 10 minute sessions are also valuable. For those with back, hip, knee and other lower body pain, consider low-impact or partial weight-bearing activities such as a recumbent bike or stepper or upright bike instead of a treadmill.
The benefits of a healthy diet are well-documented. Specifically, a Mediterranean-style diet comes highly recommended. It focuses on plenty of fruits and vegetables with fish instead of red meat and olive oil instead of butter. Researchers found people who closely adhered to a Mediterranean diet were nearly 20% less likely to have thinking and memory problems.
Exercise your brain just as you do your body. Make time each day to challenge your brain. Learn something new to keep your mind sharp. Play cards, read a book, do crossword puzzles or other word games, take a class or learn play a musical instrument.
Human beings are social animals and in the right setting, we stimulate and challenge each other. Join a book club, fitness center, or a community center. Consider volunteering, taking an art or photography class. Social interaction can prevent isolation which can lead to depression and depression is associated with dementia.
Without adequate sleep, attention and concentration is compromised. Studies show that those who have normal restful sleep outperform those who are restless and sleep deprived. Some tips for better sleep are: avoid big meals before bed, keep a consistent sleep and wake up time, avoid nicotine, caffeine and alcohol close to bedtime. “
Consider an afternoon “power nap!” Recent studies show that an afternoon nap was rejuvenating to the mind and body. Participants improved on mental skills such as memory, calculation, orientation and attention.
Cortisol is the hormone associated with stress. Recent studies have found that elevated cortisol levels were associated with poorer overall cognitive functioning, including memory, language, and processing speed.
Try yoga, massage, breathing techniques to relax. Progressive muscle relaxation (PMR) techniques can be very effective…try it on YouTube!
Smoking is clearly one of the worst things you can do to your body AND MIND! Smoking can lead to early memory lose in part due to small strokes in the brain. Do whatever it takes to quit; nicotine replacement, medication, or counseling.
There are many medical conditions and medications associated with memory loss. Regular medical check-ups can prevent, diagnose and treat some of these conditions such as; depression, diabetes, thyroid disease, vitamin deficiencies, and drug interactions or side effects. For example, sleep aid and anxiety drugs associate with memory loss.
In addition to common tricks such as word association, sticky notes, use your smart phone for appointments and reminders. If you don’t know how to use a smart phone, it is time to learn something new…and that is a healthy brain activity!
SOURCES: WebMD; Harvard Health
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

One of the greatest frustrations in modern medicine occurs when a safe, tried, and proven treatment exists to prevent deadly disease, but it is not possible to administer it to the potentially vulnerable victims. Over time, the disease unnecessarily spreads exponentially. Malaria in sub-Saharan Africa where one million die from the disease each year and tuberculosis in Haiti where the highest rate in the Western Hemisphere exists, are two examples. Another such disease that can be prevented with vaccination is the Human Papillomavirus, (HPV). While some strains of HPV lead to cancer an almost 100 percent disease prevention rate is associated with those vaccinated before the age of first potential exposure.
Despite validated scientific evidence of safety for more than 15 years, HPV vaccination skepticism not only persists, but is on the increase. Surveys show that the “anti-vaccine” culture fueled by COVID 19 has carried over to other vaccinations, including HPV. For example, provider orders for HPV vaccines decreased 24% in 2020, 9% in 2021 and 12% in 2022 when compared to 2019.
Many parents belonging to the “anti-vaccine movement” justify their actions with completely unfounded and unsupported fears of autism and other illnesses from the vaccine. However, their decisions affect the health of not only their children, but others as well.
According to Paul Offit, MD, professor of pediatrics, division of infectious diseases director of the Vaccine Education Center at the Children’s Hospital of Philadelphia (CHOP), every year in the United States, thousands of men and women die of cancers that can be prevented with a simple vaccine administered during adolescence to prevent HPV. He states, “It is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
The Centers for Disease Control (CDC) has listed the prevention of HPV as a one of its “Top 5 Health Initiatives.” The pressure will be on health care providers to take the time to educate and dispel myths in order for parents to make informed decisions for the health of their children. In fact, local pediatrician Anders Nelson, who spends significant time educating parents and children about the importance of vaccination, requires parents to sign a “Refused HPV Vaccine” form and boasts a 99% compliance rate.
2013 the CDC reported 13.9% of males and 37.6% of females’ ages 13-19 are completing vaccination for Human Papillomavirus (HPV). Despite such low vaccination rates, a 50% reduction in HPV among 14 -19-year-old females was noted. Moreover, studies demonstrate a near 100% success rate to eradicate HPV in children vaccinated between the ages of 9 and 11 years old, leading health professionals to ask a frustrating and burning question: “Why do parents hesitate to vaccinate their children from a potentially deadly virus when a safe and effective cure exists?”
Reasons cited by parents for not vaccinating are challenging to health providers. Some of the most common responses include misunderstanding of HPV and its impact, unfamiliarity with vaccine recommendations, distrust of vaccine safety, religious and moral issues with mode of disease transmission, and social pressures. It will be the purpose of this column to dispel myths and address these concerns among parents.
HPV is the most common sexually transmitted disease (STD) in the United States. It is estimated that nearly all sexually active Americans will at some point become infected with the virus. HPV is spread by direct skin to skin contact. Although the infection maybe asymptomatic, it is still possible to spread the virus. Condoms are not 100% effective to prevent HPV because infected skin may be present outside of the barrier.
Studies have demonstrated that 90 percent of sexually active males and 80 percent of sexually active females will be infected with HPV in their lifetime. Moreover, 50 percent of HPV infections are high-risk, which can lead to cancer if the body does not clear these infections.
HPV is a family of viruses that primarily produce warts, but a limited number are responsible for cancers. There are a total 120 different subtypes of the virus capable of producing warts on skin or mucus membranes. Specific strains of the virus show preference for sites of infection, and different disease progressions. For example, most types are responsible for common warts on the hands and feet, however, there are strains with a preference for producing genital/anal disease. Moreover, the HPV causing the most of significant concern are those strains responsible for certain cancers. Some HPV strains will directly interrupt a cells repair cycle, resulting in vulnerability to be transformed into a cancerous cell. HPV types 16 and 18 are high risk for cancer and account for 70% of all 490,000 cases cervical cancer with 3,900 deaths. In addition, these two types cause penile, anal and head/neck cancers.
Prevention is paramount because once infected there is no treatment for HPV infections. Only the associated lesions, including genital warts, recurrent respiratory papillomatosis (RRP), pre-cancers, and cancers are treated. Treatment options professionals utilize are biopsy, cauterization, cryotherapy, and can be mildly to severely disfiguring. Biopsy results are used to determine the HPV strain and treatment. High risk subtypes lead to increased medical observation and have the potential for more invasive treatments which can impair fertility and cause facial disfigurement.
The most popular HPV vaccine available for use is Gardasil. It has been proven to safely protect against HPV 16 and 18, which account for 70% of all cervical cancers. Gardasil additionally protects against other high and low risk virus types.
The Gardasil vaccine was initially developed in the mid 1980’s at various institutions in the US and abroad. HPV proteins were added to a previous vaccine base that was proved safe and effective. After almost 30 years of testing and scrutiny by the FDA, Gardasil was deemed safe and released to the public in 2006.
Since distribution of the Gardasil vaccine, 270 million were administered worldwide with less than .032% serious adverse events. The reported vaccine reactions are injection site discomfort, dizziness, and fainting. Furthermore, research has concluded that there is no association with neurological conditions such as Guillain-Barre’ and Autism.
Gardasil is licensed for use for males and females ages 9 through 26 years. The vaccines are administered in a series of three on a 0, 2, and 6-month schedule. Studies have shown vaccination earlier in the recommended age spectrum has more advantageous results. For example, vaccinated children between the ages of 9-11 display an almost 100% prevention of disease. Sexually activity is not a contraindication to receiving the vaccine, but the vaccine is not recommended to those currently pregnant.
Despite the safety and efficacy of the vaccines, one reason reported by parents for not vaccinating their children is the concern that vaccination will increase sexual activity in adolescents. Although disconcerting for parents, a study conducted two years before the introduction of Gardasil by the U.S. Department of Health and Human Services reported that the number of sexually active teens has increased to 30% in ages 15 to 17 and more than 63% in ages 18 to 19. Furthermore, these numbers continued to increase regardless of public programs in sexual education and abstinence.
Since released in 2006, Gardasil has made a direct impact on HPV prevalence in adolescents. Even with less than desirable vaccination rates, HPV prevalence among adolescent females age 14-19 is declining. The decline in affected teens is predicted to lead to decreased future HPV related cancers. These vaccinations are safe, effective, powerful tools at our disposal to protect our children from the detrimental effects of a preventable disease. If you would like more information on Gardasil, consult your local Family Physician, Pediatrician, or Obstetrician-gynecologists (OB/GYN). Remember the advice of CHOP pediatrician, Dr. Paul Offit regarding the HPV vaccination for adolescents, “it is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
Sources: CDC, Journal of Pediatrics, JAMA, International Journal of Cancer, Journal of Infectious Disease; www.MerckVaccines.com (GardasilR)
Medical Reviewer & Contributor: Anders Nelson, MD., F.A.A.P. is a pediatrician with offices in Scranton, PA.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
I enjoy the privilege of working with people recovering from a wide variety of medical conditions. Many of these conditions can directly affect activities of daily living, particularly, the ability to drive safely: orthopedic and sports injuries, fractures, sprains and strains, joint replacements, hip fractures, shoulder and elbow surgeries and spinal fusions. Despite the many different types of problems, there is one question that is invariably asked, “When can I return to driving?” Unfortunately, the answer is not as simple as the question because it depends on many factors. Furthermore, the implications, such as a serious accident causing further damage to the injury or surgical site or harm to someone else, are significant and possibly critical. So, the next time you ask your physician this question, please follow instructions and be patient…remember, it could be your child or grandchild running into traffic to chase a ball and you would want the driver to be at optimal function to apply the brakes!
In our culture, the inability to drive has a significant impact on lifestyle and livelihood. A study published in the Journal of Bone and Joint Surgery, found that 74% of those unable to drive due to injury or surgery are dependent on family and most of the remainder depend on friends. 4% of those unable to drive have no help at all and more than 25% suffer major financial hardship.
The report also found that family physicians, orthopedic surgeons, podiatrists, and physical therapists are keenly aware of this dilemma but often fail to communicate effectively to patients about driving. Most medical professionals express serious concerns about liability regarding return to driving following an injury or surgery. They feel that there is a lack of data to support decisions and inadequate communication among each other. They agree that they must do a better job communicating with patients and their families so they can better prepare for a period of time during their recovery in which they cannot drive.
Recent studies published in the Journal of the American Academy of Orthopaedic Surgeons (JAAOS) and the Journal of Foot and Ankle Surgery (JFAS),determined that there are two significant components in the decision of safely returning to driving after an injury or surgery; the time required for healing and the time required for a return of function. Additionally, it was found that those wearing a surgical shoe or walking boot demonstrated a significantly slower braking response time even in healthy/non-injured individuals wearing the shoe/boot.
During the time required for healing, in addition to the fear of an additional trauma from a motor vehicle accident to the healing body part, there is a general concern about the potential damage that may come from over using the body part to drive before it is adequately healed. For example, a healing fracture in the right lower leg might be compromised or delayed if one must suddenly and forcefully apply the brakes. Also, during this time, it is not unusual for post-injury or post-surgery patients to use pain medications, including narcotics. This will also compromise judgment and reaction time while driving.
Most orthopedic conditions heal in 6 to 8 weeks. However, as many of you may fully know, once a cast or splint is removed, you are not ready to run or jump. Depending on the severity of the injury, it may take many weeks of aggressive physical therapy to regain strength, range-of-motion, agility and dexterity to function at a safe level for a full return to daily activities, including driving.
The current research reinforces the fact that driving safely requires good function of the entire body. For example, just because you broke your shoulder bone but did not fracture your right leg does not mean that you are able to drive safely. Wearing a sling after arm surgery also compromises driving. First, you need a stabilized and healed injury prior to driving. Then, you must work in rehab to make modifications to return to safe driving. Apply the same scenario to injuries or surgery to the spine (neck and lower back).
*Based on research using driving simulators
7 TIPS TO KNOW WHEN YOU ARE READY TO DRIVE:
Remember, every case is unique and there is no substitute for communication with your orthopedic surgeon, podiatrist, family physician and physical therapist.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Antibiotic resistance occurs when bacteria no longer respond to the drugs designed to kill them. For more than a decade, the Centers for Disease Control along with other national and international agencies has supported an initiative called “Antibiotic Stewardship” the hallmark of which is the judicious, appropriate use of antimicrobials.
It’s told in some sobering statistics from the CDC, World Health Organization, and Food and Drug Administration:
Patients and providers must take equal responsibility. When we get sick, we often feel we need an antibiotic right away. In fact, we often demand one. A study published in the New England Journal of Medicine in 2018 found that to achieve a patient satisfaction rating in the 90th percentile physicians needed to prescribe antibiotics 75% of the time. Is this the correct approach to therapy? Are we using antibiotics too readily? What are the consequences of profuse antibiotic use?
In which of the following situations are antibiotics warranted?
A. Cold symptoms (runny nose, sore throat, headache) with a fever of 101F for 2 days
B. Cold symptoms lasting 12 days with persistent stuffiness and headache
C. Cold symptoms for 3 days with yellow-green mucous discharge
D. all of the above
The correct answer is B. Let’s discuss the reasons. Symptoms experienced as part of the common cold can include green/yellow sputum, cough, runny nose, stuffiness, sore throat, headache, fever, and mild muscle aches. This illness is caused by a virus, most likely a rhinovirus. Currently, 160 identified strains of rhinovirus are know.
Antibiotics work to destroy bacteria, not viruses since they have no activity against viruses. Antibiotics target specific bacterial structures or functions. Common bacterial targets for antibiotics include the cell wall (amoxicillin), ribosome activity (azithromycin), and bacterial DNA (levofloxacin). All of those are lacking in the very primitive structure of a virus. So, you could sit in a bathtub full of penicillin and not cure your cold with an antibiotic because there is simply nothing for the antibiotic to destroy in the viral structure.
Why are antibiotics appropriate after 10 days with cold symptoms? The typical common cold lasts between five and ten days with symptoms peaking around three or four days and waning at day six. If symptoms are consistent or regress and then become worse it is likely a sign of bacterial superinfections (super = on top of).
Usually, we carry certain bacteria with us as part of our “normal flora”. The mouth, nasal passages, large intestines, and skin host the most bacteria in the body. These bacteria work with our body and provide various “services” including protection against other more dangerous bacteria, digestion of food, and production of vitamins. A viral infection disturbs the normal balance of bacteria, allowing for proliferation and subsequent bacterial infection.
Why should we be careful about antibiotic use?
Antibiotics are not innocuous substances. They have significant side effect profiles. Adverse drug reactions associated with antibiotics can be less severe and consist of mild rash or nausea. More serious reactions include heart arrhythmias, tendon rupture, Stevens Johnson Syndrome (severe skin rash resembling thermal burns), and liver and kidney damage. Remember – every drug – not only antibiotics – has the potential to cause unpredictable adverse reactions
The most compelling reason to be careful about antibiotic use is resistance. Each time bacteria are exposed to an antibiotic, some are destroyed but others adapt to resist the antibiotic and live to see another day (remember Darwin’s Survival of the Fittest?). Antibiotics are unique in that the more they are used, the less effective they become. When antibiotics are used inappropriately – not taking them on schedule, for the right duration, taking them for a viral illness – bacteria have a chance to adapt to overcome the antibiotic activity. The resistant bacteria may go on to set up a resistant infection in you or that bacteria may be transmitted to others.
There are several ways we can combat this problem according to the Joint Commission on Healthcare Accreditation 2020 Standards. It is important to identify the causative agent if possible.
For example, a sore throat should not be treated with antibiotics until a throat culture or rapid strep test is obtained and a bacterial cause is identified. According to the Infectious Disease Society of America, 90 percent of adult sore throats have a viral cause, not bacterial. Avoid unneeded clinic or urgent care visits and utilize OTC and non-drug measures to manage non-bacterial infection symptoms.
Mislabeled allergy status leads to more expensive, less optimal antibiotic choices, more complex administration, increased resistance rates, and more treatment failures. The most common listed drug allergy in the US is Penicillin. According to the CDC, 10% percent of patients reports an allergy, however, < 1% of patients have a true allergy precluding penicillin or penicillin-like agents (the biggest class of antibiotic agents).
Vaccines may prevent bacterial infections or prevent viral infections which will avert a bacterial superinfection. Here are two examples of where vaccines can lower antibiotic use. The pneumococcal “pneumonia” vaccine protects against the bacterium Streptococcus pneumoniae. Following the current guidelines for vaccination during childhood and adulthood decreases pneumococcal infections. According to the CDC, this vaccine has reduced pneumococcal infections by more than 90% in children. In addition, antibiotic-resistant pneumococcal infections have decreased in the United States since the pneumococcal vaccine was introduced.
The shingles vaccine also minimizes antibiotic use. The shingles vaccine “Shingrix”, is currently approved for individuals 50 years old (and older) as a two-dose series. Not only does it effectively prevent the occurrence of shingles, a painful, debilitating re-emergence of the chickenpox virus, but also reduces the risk of a potential secondary bacterial skin superinfection. Vaccine prevention of viral illness may subsequently eliminate antibiotic use.
Educating patients and prescribers will lead to the proper use of antibiotics to curb antibiotic resistance.
Guest Author: Dr. Gretchen Welby, PharmD, MHA
Dr. Welby received degrees from Keystone College and Philadelphia College of Pharmacy and Science. She received a Master of Health Administration Degree from the University of Scranton and a Doctor of Pharmacy degree from Temple University. She is currently the Academic Director of the Physician Assistant Program at Marywood University where she teaches Anatomy, Physiology, Pathophysiology, and Pharmacology.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from patients and sports fans about the nature of the Achilles Tendon rupture injury, recovery, and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to warm-up and exercise during the winter months. A little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears, especially Achilles Tendon rupture. The Achilles tendon is one of the more common tendons torn.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for tendons completely torn, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return to close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
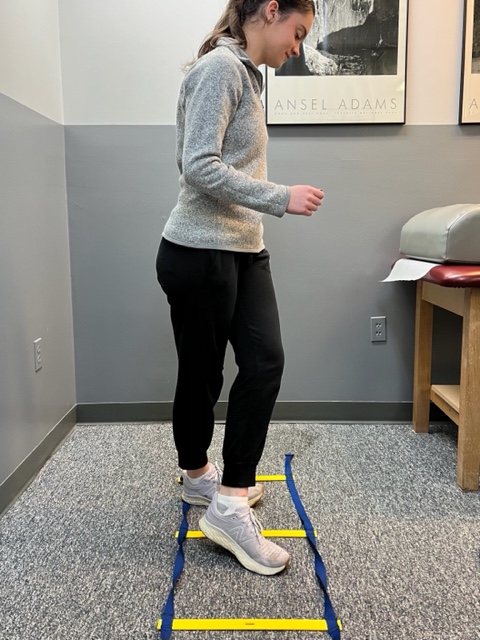
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes: gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity – Photo 1) and proprioceptive and agility drills are essential (Photos 2 & 3).


In PHOTO 1a & 1b: Eccentric Lowering and Lengthening: for the Achillies tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
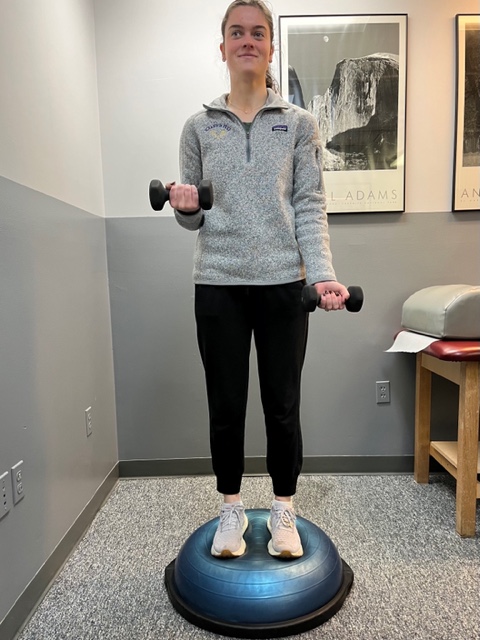
In PHOTO 2: Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
PHOTO 3: Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.
MODEL: Kerry McGrath, student physical therapy aide at Mackarey Physical Therapy
Sources: MayoClinic.com;Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
Research shows, those who prepare in advance for their physician visits, have more satisfaction than those who just show up for their appointment. Moreover, for patients seeing multiple physicians, such as specialists, often communication is poor and your participation in the process can be invaluable. There are things you can do to prepare for your physician visits:
Remember, your health is too important to rely on memory for accuracy…so be a proactive participant. With technology, it has never been easier to keep a medical journal to improve accuracy and communication. There are several “Apps” such as “mymedicalapp.com” that allow you to do this on your phone, tablet or lap-top computer and offer privacy code features.
SOURCES: www.webmd.com; National Institutes of Health – National Institute on Aging “A Guide for Older People - Talking With Your Doctor”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician.
For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit: http://www.mackareyphysicaltherapy.com/forum
“I was nervous and forgot to ask my doctor questions about my diagnosis!” “When the nurse asked me, I could not remember my medications!” These are two examples of the many frustrations patients have when visiting their physicians. Research shows, those who prepare in advance for their physician visits, have more satisfaction than those who just show up for their appointment. Moreover, for patients seeing multiple physicians, such as specialists, often communication is poor and your participation in the process can be invaluable. There are things you can do to prepare for your physician visits...
Remember, your health is too important to rely on memory for accuracy…so be a proactive participant. With technology, it has never been easier to keep a medical journal to improve accuracy and communication. There are several “Apps” such as “mymedicalapp.com” that allow you to do this on your phone, tablet or lap-top computer and offer privacy code features.
SOURCES: www.webmd.com; National Institutes of Health – National Institute on Aging “A Guide for Older People - Talking With Your Doctor”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit https://mackareyphysicaltherapy.com/forum/
