Happy Holidays! Despite political divisions and war in the Middle East and Ukraine, it is at this time of year that we celebrate life with great hope and faith. People of many faiths take time to reflect, respect, and resolve. Christians celebrate Christmas, the miraculous birth of Christ, the Son of God, and the Messiah. Jews celebrate Chanukah, the miraculous festival of lights, when one night’s oil provided enough light and safety for 8 nights. Both major faiths promote healthy lifestyles for the mind, body and spirit. These faiths are grounded in hope, faith, love and peace. It is no surprise that studies repeatedly demonstrate that faithful and spiritual people live longer and healthier lives! At this turbulent time in the world, it is important to note that people of all faiths benefited equally!
I purport, that to be truly healthy, one must have faith because complete health is multidimensional. Socrates preached this message to his students thousands of years before Christ. One must have a healthy mind, which requires intellectual stimulation with attainable goals related to education and intellect. One must have a healthy body by eating well, engaging in physical activity and having attainable goals related to his/her body. Likewise, one must have a healthy spirit with faith, hope, prayer and meditation, comrades and counsel, and set attainable spiritual goals.
How being religious or spiritual has been shown to benefit your mind, body and spirit…
1. Healthy Blood Pressure: High blood pressure (hypertension) can lead to heart disease and stroke, which are the leading causes of death in the United States, according to the Centers of Disease Control (CDC). It affects 1 in every 3 adults and only half of these people have their blood pressure under control. Well, religion and spiritually may help …
The health benefits of religion or spirituality are well documented. One study conducted at Duke University Medical Center on 4,000 subjects, older adults who described themselves as religiously active were 40% less likely to have high blood pressure when compared to those less active. Moreover, they were surprised to find that those who described themselves as spiritual rather than religious also were less likely to develop high blood pressure.
2. Greater Sense of Satisfaction: Research also indicates that religious people are more satisfied with their lives than those without faith. A sociology study determined that high satisfaction among church goers may be due to the strong social bonds that are developed within a religious congregation. Regular church attendees see the same people weekly and often more often, when participating in rewarding and gratifying church-related volunteer work.
3. Greater Tolerance for Adversity: In an impressive study published in the Journal of the American Medical Association, researchers interviewed 345 late-stage cancer patients to assess their spirituality as it related to their illness. 88% stated that they were religious as it related to their coping mechanisms. It was determined that those using religion for coping demonstrated a 7.4% rate of resuscitation as compared to 1.8% for those not using religion as a coping mechanism.
4. Stronger Immune System: According to a Duke University study of 1,718 older adult participants, those described as “highly spiritual” were 50% less likely to have high levels of anti-inflammatory proteins that weaken the immune system and have been linked to some cancers, viral infections and autoimmune diseases. The outcome was similar for those who attend religious services at least once a week.
5. Greater Longevity Those who attend religious services more than once per week are found to live and additional 7 years when compared to those who never attend services. Again, researchers feel that the social benefits of a belonging to a strong religious community may be a large part of the associated longevity. Additionally, the lifestyle of religious people is often healthier: members of these communities rarely engage in risky and unhealthy behaviors such as smoking, excessive drinking, indiscriminate sex, etc
Visit your doctor regularly and listen to your body.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Holiday shopping is stressful for your body, causing backache, as well as your wallet. Even the “online shopper” is at risk when you consider the hours sitting with poor posture on your electronic device. But I do believe that “in person” shopping is worse for backache… driving from store to store, getting in and out of the car while bundled in a sweater and winter coat can add stress to your spine. Often, the expert shopper carries package after package from the store to the car, repeatedly. Six, eight, or ten hours later, the shopper arrives home exhausted with the backache slowly increasing, only to realize that 15 or 20 packages must be carried from the car into the house. This dilemma is compounded by the fact that the rain turned to sleet, and the sleet to snow. You are slipping and sliding all the way from the car to the house while carrying multiple packages of various sizes and shapes, fighting through the already developing backache. The shopping bags get wet and tear, forcing you to tilt your body as you carry the packages. Of course, no one is home to help you unload the car and you make the trip several times alone. You get into the house exhausted and crash onto the couch because your backache is too much to do anymore at this point. You fall asleep slouched and slumped in an overstuffed pillow chair. Hours later you wake up with a stiff neck and lower back pain. You wonder what happened to your neck and back.
Plan Ahead: It is very stressful on your spirit, wallet and back to do all of your shopping in the three weeks available after Thanksgiving. Even though we dislike “rushing” past Thanksgiving to the next holiday, try to begin holiday shopping in before
Use the Internet: Supporting local businesses is important. However, Internet shopping can save you lots of wear and tear. Sometimes, you can even get a gift wrapped.
Gift Certificates: While gift certificates may be impersonal, they are easy, convenient and can also be purchased over the internet.
Perform Stretching Exercises: Stretch intermittently throughout the shopping day…try the three exercises below, gently, slowly, hold 3 seconds and relax, repeat 5 times.



Model: Paul Mackarey, PT, DPT, Clinic Director, Mackarey PT
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

While I normally do not address the topic of shoveling snow until January, considering recent weather events, I thought it might be valuable to present it sooner. Much has been written about the dangers of snow shoveling for your heart. However, while not fatal, low back pain is the most common injury sustained while shoveling snow. Heart attacks are also more common following wet and heavy snow.
Snow shoveling can place excessive stress on the structures of the spine. When overloaded and overstressed, these structures fail to support the spine properly. The lower back is at great risk of injury when bending forward, twisting, lifting a load, and lifting a load with a long lever. When all these factors are combined simultaneously, as in snow shoveling, the lower back is destined to fail. Low back pain from muscle strain or a herniated disc is very common following excessive snow shoveling.
Sources: The Colorado Comprehensive Spine Institute; American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

The “first Thanksgiving” was in 1621 between the Pilgrims of Plymouth Colony and the Wampanoag tribe in present day Massachusetts to celebrate the harvest and other blessings of the previous year. In 1789, President George Washington, at the request of Congress, proclaimed Thursday, November 26, as a day of national thanksgiving. In 1863, Abraham Lincoln proclaimed the national holiday of Thanksgiving to be the last Thursday of November.
Americans and Canadians continue to celebrate this holiday as a time for family and friends to gather, feast, and reflect upon their many blessings. Like most, I am very grateful for the simple things; family, good friends, food, shelter, and health. It turns out that being grateful is, not only reflective and cleansing; it is also good for your health!
Grateful people are more likely to behave in a prosocial manner, even when it is not reciprocated. A study by the University of Kentucky found those ranking higher on gratitude scales were less likely to retaliate against others, even when others were less kind. Emmons and McCullough conducted one of the most detailed studies on thankfulness. They monitored the happiness of a group of people after they performed the following exercise:
There are many things in our lives, both large and small, that we might be grateful about. Think back over the past week and write down on the lines below up to five things in your life that you are grateful or thankful for.” The study showed that people who are encouraged to think of things they’re grateful for are approximately 10% happier than those who are not.
Amy Morin, psychotherapist, mental health trainer and bestselling author offers this advice: “Developing an “attitude of gratitude” is one of the simplest ways to improve your satisfaction with life. We all have the ability and opportunity to cultivate gratitude. Simply take a few moments to focus on all that you have, rather than complain about all the things you think you deserve.” So…be grateful and have a happy Thanksgiving!
Source: NIH, Forbes, Amy Morin “13 Things Mentally Strong People Don’t Do.”
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

November is National Hospice Month! During this time, we celebrate the tireless work of the hospice professionals who assist patients and their families during the weeks and months that they journey with a serious or terminal illness.
However, in addition to the service of providing pain and symptom management, assisting with personal care, providing volunteer, counseling and social work services, there may be many other services that your local hospice program may be able to offer to patients, families and caregivers alike.
Please keep in mind that each hospice agency provides unique services to the community. Before you decide, it is important to reach out and ask which agency offers services that best meet your needs.
Some community support programs that are offered by hospice agencies that are routinely available include:
Bereavement Support ---Dealing with the death of a loved one can be a difficult and often lonely endeavor. All hospice agencies offer bereavement services to families of patients that have died. In addition, many hospices offer community support programming to help those who have suffered a loss. Some support programs are in groups, but often individualized help is available. Most times the bereavement services for the community are without charge.
Pet Bereavement Support---The death of a pet can often be quite traumatizing, especially when the pet has been a long-standing member of the family. Hospice agencies are offering bereavement counseling for those who suffered the loss of a pet. Call and reach out if you have suffered a loss and require support.
Dementia Support Groups--- Nancy Reagan always referred to the diagnosis of President Reagan as the ‘long goodbye’. Dealing with a loved one suffering with dementia is difficult---but you do not have to deal with this alone. Many hospices have dementia support groups that educate, support and guide.
Supporting Children through a Loss---Often it is difficult for children to understand or process the death of a parent, sibling, and grandparent or loved one. There are specialized programs for children to understand and live with the loss----developing a new normal. These programs are usually done in a series of 5 sessions so that proper education and guidance can be accomplished.
Community Education Series--- Not only are your local hospices taking the lead to advance end of life care, but many are helping to educate the professional and lay community alike. Ask about monthly seminars, educational programs and other topics of interest to you and your family/co-workers.
Memorial Services--- Hospice agencies routinely celebrate the lives of those patients who have died within the last 6 months or a year. Surrounding yourself with others who have suffered a loss can often be healing and certainly supportive. Call and ask your local hospice about planned memorial services that honor lives well lived through prayer and testimonials.
Volunteer opportunities---There can be no better way to give back to your community than through volunteering opportunities. Hospice offers a wide array of ways to volunteer ranging from direct patient contact to more administrative tasks. Whatever the job, the act of volunteering is what makes hospice care so special.
Mentoring Programs--- As hospice programs are traditionally interdisciplinary in approach; students working with hospice programs are provided an optimal environment to learn not only hospice care, but also the ever-important concept of team. Many hospice agencies work with students regularly from nursing schools, universities and our local medical college.
Transitions Program--- Often patients are referred for hospice services, but do not meet eligibility requirements for this level of care. However, many hospice agencies offer a transitions program, which is a volunteer supported program to monitor the frail elderly in the community and reporting changes back to the physician for advice and guidance. These programs are free of charge, volunteer supported and a valuable asset for the independent senior who may need that extra set of eyes and ears of a skilled volunteer.
So, in honor of National Hospice Month, we say, thank you to all the hospice professionals, volunteers and families who work so diligently to care for those in our community with a serious or terminal illness. But remember too, that your local hospice agency can be a wonderful resource for education, mentoring, dementia support and grief counseling. Ask questions, attend a seminar, inquire about memorial services or look for support when caring for a loved one with dementia. Help, support, guidance and education are available----just make the call to your local hospice agency.
To find out which hospices serve your community, call NHPCO’s HelpLine at 1-800-658-8898 or visit www.caringinfo.org/findahospice.
Medical Contributor: Ralph DeMario, MD, Former CMO, Hospice of the Sacred Heart
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

November is National Hospice Month! Each November, the community of hospice and palliative care professionals celebrates National Hospice Month. Although, at first glance, spotlighting the concept of death and dying may seem a bit gloomy. It’s actually the concept of quality of life and the focus on living that is truly being celebrated.
It is true that hospice serves those patients and their families who are on the journey of a serious or terminal illness. But as any hospice professional from the nurse to the social worker to the volunteer to the pastoral counselor will attest------our focus is ALWAYS on the value of life being maintained and the quality of living for each and every one of our patients.
Placing the focal point of hospice care on living, instead of dying, enables the patient and family to focus on:
Remember that your hospice team will make suggestions to improve your pain and symptoms, all with the ultimate goal of allowing you to live your life as fully and functionally as possible. Pain alleviation will allow for improved activities, help with personal care will conserve energy for visiting with family and friends, and allowing a volunteer into your home will give caregivers much needed time for rest and relaxation.
There are a number of myths surrounding hospice care----and this is good a time as ever to help dispel them…
Myth #1--- Hospice is for patients in the last days of their lives.
Actually, hospice care was designed to care for patients and their families for the last 6 months of their lives----the longer patients are under the care of hospice professionals, the better their symptoms are controlled and the better their quality of living.
Myth #2--- Pain medications are given in large doses to sedate the patient and hasten death…..
Pain medications are used in small of doses as required to control pain, and to maintain patients’ alertness, always focusing on living life to the fullest. Medications are never given to hasten death, only to control pain and maintain quality of life.
Myth #3--- Once patients start hospice services, death will come soon….
The statistics on this issue are interesting. In a major study, patients who received hospice care for congestive heart failure actually lived 29 days longer!!! Also, on average 15% of patients are actually discharged from hospice services because of significant improvement in symptoms.
Myth #4--- Patients receiving hospice services cannot leave the home or travel….
The truth is that patients receiving hospice care can drive, travel as able, go to bingo/hairdresser/casino----actually come and go as they are able. So the goal is to improve symptoms so that patients can enjoy their lives as fully as possible while on the journey of a serious illness.
Although the topic of death and dying has been rather taboo in the US, hospice professionals celebrate the living potential that their patients still have. The focus is on quality of relationships, maintaining a functional lifestyle and living the life they were meant to live. Hospice professionals also celebrate the many lives they have improved, all the lives they have touched and the fact that they were chosen to dedicate their professional lives to helping others live more fully……
To find out which hospices serve your community, call NHPCO’s HelpLine at 1-800-658-8898 or visit www.caringinfo.org/findahospice
Medical Contributor: Ralph DeMario, MD, Former CMO, Hospice of the Sacred Heart
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.comPaul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Recently, two patients asked me when I thought it would be safe for them to return to their exercise programs after abdominal surgery. She stated that she was not sure how to properly and safely implement or return to her program.
This column will attempt to ensure a safe return to activity and exercise following general surgery such as gall bladder, appendix, hernia, etc. The post-operative patient has many questions: When is it safe to begin an exercise program? How do I begin? What is the best exercise? Which exercises are best? How do I know if the activity is too intense or not intense enough? Are there safe guidelines?
Before you begin, discuss your intention to exercise with your surgeon and primary care physician. Get medical clearance to make sure you can exercise safely. With the exception of short daily walks, don’t be disappointed if your surgeon requires you to wait at least until your 6 week post-op check-up to begin exercise.
While a 60 minute workout would be the long term goal, begin slowly at 15-20-30 minutes and add a few minutes each week. Make time to warm up and cool down.
Warm-up 5-10 minutes
Strength Training 10-15-20 minutes
Aerobic 10-15-20 minutes
Cool down 5-10 minutes
How to Monitor Your Exercise Program:
First, determine your resting heart rate by taking your HR (pulse) using your index finger on the thumb side of your wrist for 30 seconds and multiply it by two. 80 beats per minute is considered a normal HR but it varies. This is a good baseline to use as a goal to return to upon completion of your workout. For example, your HR may increase to 150 during exercise, but you want to return to your pre exercise HR (80) within 3-5 minutes after you complete the workout.
For those who are healthy, calculating your target heart rate (HR) is an easy and useful tool to monitor exercise intensity.
220 – Your Age = Maximum Heart Rate
EXAMPLE for a 45 year old: 220 – 45 = 175 beats per minute should not be exceeded during exercise.
For those concerned about calories expended during exercise.
NOTE: Keep the level at a light/moderate level for the first four to six weeks and advance to the moderate/heavy at week six. The Very Heavy Level may not be appropriate for 12 weeks post op is for those who have a reasonable fitness level and exercise 4-5 days per week.
Example of Data Found on Fitness Equipment
Remember, this is only accurate if you program your correct height, weight and age.
Level kCal/min MET
Light 2 - 4.9 1.6 – 3.9
Moderate 5 - 7.4 4 – 5.9
Heavy 7.5 - 9.9 6 - 7.9
Very Heavy 10 - 12.4 8 – 9.9
Always secure physician approval before engaging in an exercise program.
If the patient is on beta blockers (Atenolol, Bisoprolol, etc), it is important to use the Borg Rating of Perceived Exertion Scale (RPE) scale to determine safe exercise stress since exercise will not increase HR as expected:
0 - Nothing at all
1 - Very light
2 - Light
3 - Moderate
4 - Somewhat intense
5 - Intense (heavy)
6
7 - Very intense
8
9 - Very, very intense
10 - Maximum Intensity
NOTE: Keep the RPE at 2-3 the first 6 weeks post op and advance to level 3-4 at 8-12 weeks post op. Levels 5-6-7 are for those with a reasonable fitness level and exercise 4-5 days per week. The advanced levels should not be attained until 2-3 months of exercise and 3-4 months post op.
MEDICAL CONTRIBUTOR: Timothy Farrell, MD, is a general surgeon at GCMC.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Osteochondritis dissecans, also called OCD, is the most common cause of a loose body or fragment in the knee and is usually found in young males between the ages of ten and twenty. While this word sounds like a mouth full, breaking down its Latin derivation to its simplest terms makes it understandable: “osteo” means bone, “chondro” means cartilage, “itis” means inflammation, and “dissecans” means dissect or separate. In OCD, a flap of cartilage with a thin layer of bone separates from the end of the bone. As the flap floats loosely in the joint, it becomes inflamed, painful and disrupts the normal function of the joint.
Typically, OCD is found in the knee joint of active young men who participate in sports which involve jumping or full contact. Although less common, it is also found in other joints such as the elbow.
Often, the exact cause of OCD is unknown. For a variety of reasons, blood flow to the small segment at the end of the bone lessens and the weak tissue breaks away and becomes a source of pain in the joint. Long term, OCD can increase the risk of osteoarthritis in the involved joint.
To properly diagnose OCD a physician will consider onset, related activities, symptoms, medical history, and examine the joint involved for pain, tenderness, loss of strength and limited range of motion. Often, a referral to a specialist such as an orthopedic surgeon for further examination is necessary. Special tests specifically detect a defect in the bone or cartilage of the joint such as:
Radiograph (X-ray) may be performed to assess the bones.
Magnetic Resonance Imaging (MRI) may be performed to assess bones and other soft tissues such as cartilage, ligaments, muscles and tendons.
The primary goal of treatment for OCD is to relieve pain, control swelling, and restore the complete function (strength and range of motion) of the joint. The age of the patient and severity of the injury determine the treatment methods. For example, medications assist with pain and inflammation reduction.
Young patients who are still growing have a good chance of healing with conservative treatment. Rest and physical therapy are the conservative treatments of choice. Rest entails avoiding any activity that compresses the joint such as jumping, running, twisting, squatting, etc. In some cases, using a splint, brace and crutches to protect the joint and eliminate full weight bearing, may be necessary for a few weeks. Physical therapy, either as a conservative or post operative treatment, involves restoring the range of motion with stretching exercises and improving the strength and stability of the joint through strengthening exercises. Modalities for pain and swelling such as heat, cold, electrical stimulation, ultrasound, compression devices assist with treatment depending on the age of the patient and severity of the problem.
Conservative treatment can often require 3 to 6 months to be effective. However, if it fails, arthroscopic surgery stimulates healing or reattaches the loose fragment of cartilage and bone. In some cases if the defect is small, surgery involves filling in the defect with small bundles of cartilage. In other cases, the fragment is reattached directly to the defect using a small screw or bioabsorbable device. More recently, surgeons are using the bone marrow of the patient to repair the deficit by stimulating the growth of new tissue (bone marrow stimulation).
In other cases, a plug of healthy tissue from the non-weight bearing surface of a patient's knee relocated to the defect to stimulate healing (osteochondral autograft transplantation OATS). While there are many surgical options for OCD, an orthopedic surgeon will help the patient decide the most appropriate procedure based on age, size of defect, and other factors.
While prevention is not always possible, some measures can be taken to limit risk. For example, if a child playing sports has a father and older brother who had OCD, then it would be wise to consider the following: Avoid or make modifications for sports requiring constant jumping. Cross-train for a sport to avoid daily trauma (run one day and bike the next). Also, do not play the sport all year round (basketball in the fall/winter and baseball in the spring/summer). Seek the advice from an orthopedic or sports physical therapist to learn proper strength and conditioning techniques. Learn proper biomechanics of lifting, throwing, squatting, running, jumping and landing.
Sources: Mayo Clinic
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Fall has arrived in NEPA and walking is a great way to enjoy the fall foliage. Moreover, a new study has found that walking can reduce lower back pain. Researchers in Australia followed more than 700 adults who had a recent onset of lower back pain (and were able to bear full weight without associated leg symptoms) and enrolled them in a walking program under the supervision of a physical therapist. One group walked for 30 minutes, 3-5 times per week and the control group remained inactive. Both groups were followed for more than three years and discovered that the inactive control group was twice as likely to suffer from repeated flare-ups of lower back pain when compared to the walking group.
It is good news for those who enjoy walking, however, for many who have not maintained an active lifestyle or have health issues, it is challenging to know where to begin. Also, beginning without a good plan can lead to injury and leave you discouraged. For example, those overweight and de-conditioned should not start a walking program too aggressively. Walking at a fast pace and long distance without gradually weaning yourself into it will most likely lead to problems.
There is probably nothing more natural to human beings than walking. Ever since Australopithecus, an early hominin (human ancestor) who evolved in Southern and Eastern Africa between 4 and 2 million years ago, our ancestors took their first steps as committed bipeds. With free hands, humans advanced in hunting, gathering, making tools etc. while modern man uses walking as, not only a form of locomotion, but also as a form of exercise and fitness. It is natural, easy and free...no equipment or fitness club membership required!
Walking to reduce or control lower back pain is only one of many important reasons to begin a program. According to the American Heart Association, walking as little as 30 minutes a day can provide the following benefits:
Anything is better than nothing! However, for most healthy adults, the Department of Health and Human Services recommends at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity, or an equivalent combination of moderate and vigorous aerobic activity. The guidelines suggest that you spread out this exercise during the course of a week. Also aim to do strength training exercises of all major muscle groups at least two times a week.
As a general goal, aim for at least 30 minutes of physical activity a day. If you can't set aside that much time, try several short sessions of activity throughout the day (3 ten or 2 fifteen-minute sessions). Even small amounts of physical activity are helpful, and accumulated activity throughout the day adds up to provide health benefit.
Remember it's OK to start slowly — especially if you haven't been exercising regularly. You might start with five minutes a day the first week, and then increase your time by five minutes each week until you reach at least 30 minutes.
For even more health benefits, aim for at least 60 minutes of physical activity most days of the week. Once you are ready for a challenge, add hills, increase speed and distance.
Keeping a record of how many steps you take, the distance you walk and how long it takes can help you see where you started from and serve as a source of inspiration. Record these numbers in a walking journal or log them in a spreadsheet or a physical activity app. Another option is to use an electronic device such as a smart watch, pedometer or fitness tracker to calculate steps and distance.
Make walking part of your daily routine. Pick a time that works best for you. Some prefer early morning, others lunchtime or after work. Enter it in your smart phone with a reminder and get to it!
Studies show that compliance with an exercise program is significantly improved when an exercise buddy is part of the equation. It is hard to let someone down or break plans when you commit to someone. Keep in mind that your exercise buddy can also include your dog!
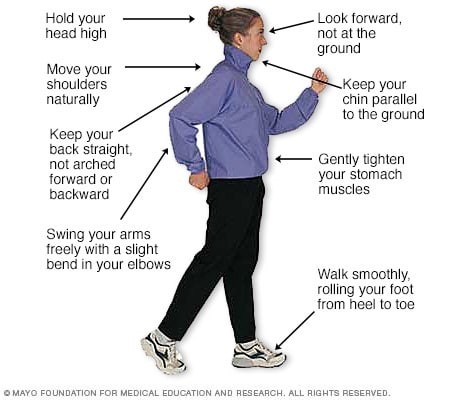
Like everything, there is a right way of doing something, even walking. For efficiency and safety, walking with proper stride is important. A fitness stride requires good posture and purposeful movements. Ideally, here's how you'll look when you're walking:
Sources : Sapiens.org; WebMD; Mayo Clinic, “Health & Science New”
Visit your doctor regularly and listen to your body
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Age-related changes to your body are normal and expected. For example, loss of muscle tone, stiffness in joints, and loss of balance. With effort, some of these changes can be retarded and managed with stretching, strengthening and balance exercises. The brain is no different…it can slow down and lead to memory lapses. However, for most of us, it too can be managed and with a little effort, be kept sharp and clear.
Many experts feel that exercise is the best method to maintain not only physical health but mental health. Regular exercise can prevent the things that contribute to memory loss with age such as; diabetes, high blood pressure, high cholesterol, obesity and stroke.
Specifically, aerobic exercise may be most beneficial. Aerobic exercise is any type of sustained exercise that strengthens the heart and lungs to improve the body’s use of oxygen. This may include running/jogging, brisk walking, cycling, swimming, rowing, and the use of a treadmill, elliptical, stepper or similar device, at light to moderate intensity which requires the use of oxygen to adequately meet the oxygen demands of the body for an extended period of time. The generally accepted time and frequency is at least 30 minute sessions performed three or more times per week. Two 15 minute or three 10 minute sessions are also valuable. For those with back, hip, knee and other lower body pain, consider low-impact or partial weight-bearing activities such as a recumbent bike or stepper or upright bike instead of a treadmill.
The benefits of a healthy diet are well-documented. Specifically, a Mediterranean-style diet comes highly recommended. It focuses on plenty of fruits and vegetables with fish instead of red meat and olive oil instead of butter. Researchers found people who closely adhered to a Mediterranean diet were nearly 20% less likely to have thinking and memory problems.
Exercise your brain just as you do your body. Make time each day to challenge your brain. Learn something new to keep your mind sharp. Play cards, read a book, do crossword puzzles or other word games, take a class or learn play a musical instrument.
Human beings are social animals and in the right setting, we stimulate and challenge each other. Join a book club, fitness center, or a community center. Consider volunteering, taking an art or photography class. Social interaction can prevent isolation which can lead to depression and depression is associated with dementia.
Without adequate sleep, attention and concentration is compromised. Studies show that those who have normal restful sleep outperform those who are restless and sleep deprived. Some tips for better sleep are: avoid big meals before bed, keep a consistent sleep and wake up time, avoid nicotine, caffeine and alcohol close to bedtime. “
Consider an afternoon “power nap!” Recent studies show that an afternoon nap was rejuvenating to the mind and body. Participants improved on mental skills such as memory, calculation, orientation and attention.
Cortisol is the hormone associated with stress. Recent studies have found that elevated cortisol levels were associated with poorer overall cognitive functioning, including memory, language, and processing speed.
Try yoga, massage, breathing techniques to relax. Progressive muscle relaxation (PMR) techniques can be very effective…try it on YouTube!
Smoking is clearly one of the worst things you can do to your body AND MIND! Smoking can lead to early memory lose in part due to small strokes in the brain. Do whatever it takes to quit; nicotine replacement, medication, or counseling.
There are many medical conditions and medications associated with memory loss. Regular medical check-ups can prevent, diagnose and treat some of these conditions such as; depression, diabetes, thyroid disease, vitamin deficiencies, and drug interactions or side effects. For example, sleep aid and anxiety drugs associate with memory loss.
In addition to common tricks such as word association, sticky notes, use your smart phone for appointments and reminders. If you don’t know how to use a smart phone, it is time to learn something new…and that is a healthy brain activity!
SOURCES: WebMD; Harvard Health
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

