It is two weeks away from the 28th Steamtown Marathon. After training all spring and summer for the first seven Steamtown Marathons, not a Columbus Day Weekend goes by without my thoughts of this great event.
I would like to introduce this topic with some marathon history. In 490 B.C. Athens was under attack by the Persians and was outnumbered more than two to one. The Athenians fought bravely and defeated the enemy in the town of Marathon. The victory kept the intruders 26 miles away from Athens. To keep the anxious citizens of Athens calm, leaders immediately ordered a foot soldier, Phedippides, to run to the capital city to share the news. Phedippides ran, in full armor, for 26 miles from Marathon to Athens, delivered the message and died immediately. Now, people do the same thing of their own free will!
Each year at this time, dozens of runners preparing for the Steamtown Marathon come to my office with severe shin pain known as shin splints. Unfortunately, in many of these athletes, this problem can lead to a much more severe and advanced problem with shin splints called a stress fracture.
A stress fracture is fatigue damage to bone with partial or complete disruption of the cortex of the bone from repetitive loading. While standard x-rays may not reveal the problem, a bone scan, and MRI will. It usually occurs in the long bones of the leg, mostly the tibia but also the femur (thigh) and foot. Occasionally, it occurs in the arm.
10-21% of all competitive athletes are at risk for stress fractures. Track, cross country and military recruits are at greatest risk. Females are twice as likely as males to have a stress fracture. Other athletes at risk are: sprinters, soccer and basketball players, jumpers, ballet dancers are at risk in the leg and foot. Gymnasts are also vulnerable in the spine while rowers, baseball pitchers, golfers and tennis players can experience the fracture with much less frequency in the ribs & arm.
The problem is much more prevalent in weight bearing repetitive, loading sports in which leanness is emphasized (ballet, cheerleading) or provides an advantage (distance running, gymnastics).
Stress fractures usually begin with a manageable, poorly localized pain with or immediately after activity such as a shin splint. Over time, pain becomes more localized and tender during activity and then progresses to pain with daily activity and at rest.
Visit your doctor regularly and listen to your body.

Read Health & Fitness Forum Next Monday/Sunday: Preparing Your First Aid Kit For the Steamtown Marathon
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Despite recent challenges for air travel due to increased volume, severe weather and a nationwide shortage of air traffic controllers, Americans report high levels of enthusiasm for air travel this summer, including travel abroad.
Confession; I recently was on a long trip that required sitting on an airplane for more than six hours…and I wore compression stockings … guess I’m getting older (and wiser)!
Have you noticed that being in a car or on an airplane for more than three hours leads to neck and back pain? Soreness, stiffness and swelling in your legs? With a little planning, preventing or limiting these problems on long trips is possible. Also, as people age and/or develop other health problems, they are more vulnerable to developing a more serious problem associated with long trips; deep vein thrombosis (DVT) or blood clots. But problems with long-distance travel can be avoided. The following tips, based on research and personal experience, can prevent neck, back and leg pain and stiffness and DVT.
A DVT is a blood clot that forms in a deep vein. The deep veins pass through the muscles and cannot be seen like the veins just under your skin. While it may occur in your arms, it is much more common in the legs, especially the calf muscle when traveling. When a blood clot forms in a leg vein it usually sticks to the vein wall. Often, pain and swelling lead you to the doctor and treatment is rendered before serious complications develop. However, there are two possible complications. One, a pulmonary embolus, occurs when a part of the clot logged in your deep vein of the calf breaks off and gets lodged in the lung. This is a very serious problem that can be fatal. Two, post-thrombotic syndrome, occurs when you have pain and swelling in your calf after a DVT.
The following risk factors for DVT significantly increase the potential for problems when traveling on long trips by air, more than 5 hours. Trains, cars and buses also create a risk, but air travel creates a greater risk for the following reasons: reduced cabin pressure, reduced cabin oxygen levels, dehydration and alcoholic drinks, which may increase dehydration and immobility.
Airplane seats are “C” shaped and force you to round your neck and back forwards. These exercises are designed to stretch and extend your back in the opposite direction. Please perform slowly, hold for 3-5 seconds and repeat 10 times each hour.
Sitting:
When sitting in an airplane seat, take the neck pillow in the overhead compartment and place it in the small of your lower back. While sitting or standing up, perform postural exercises every 30-45 minutes.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

I have been advising my patients to exercise, keep active, and walk as long as they can in order to stay mobile and healthy. However, seniors often tell me activities that require prolonged walking is limited by ankle pain from arthritis. They often ask, “What is arthritis of the ankle?” How does it happen? What can I do about it?
Your family physician will examine your ankle to determine if you have arthritis. In more advanced cases you may be referred to a specialist such as a podiatrist, orthopaedic surgeon or rheumatologist for further examination and treatment. X-rays will show if the joint space between the bones in the ankle is getting narrow from wear and tear arthritis. If rheumatoid arthritis is suspected, blood tests and an MRI may be ordered. The diagnosis will determine if you problem if minor, moderate or severe.
In the early stages your treatment will be a conservative, nonsurgical approach, which may include; anti-inflammatory medication, orthopedic physical therapy, exercise, activity modifications, supplements, bracing, etc. You and your family physician, podiatrist, orthopedic surgeon or rheumatologist will decide which choices are best.
When conservative measures no longer succeed in controlling pain and deformity, improving strength and function then more aggressive treatment may be necessary.
SOURCES: Rothman Institute, Philadelphia, PA and American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
I enjoy the privilege of working with people recovering from a wide variety of medical conditions. Many of these conditions can directly affect activities of daily living, particularly, the ability to drive safely: orthopedic and sports injuries, fractures, sprains and strains, joint replacements, hip fractures, shoulder and elbow surgeries and spinal fusions. Despite the many different types of problems, there is one question that is invariably asked, “When can I return to driving?” Unfortunately, the answer is not as simple as the question because it depends on many factors. Furthermore, the implications, such as a serious accident causing further damage to the injury or surgical site or harm to someone else, are significant and possibly critical. So, the next time you ask your physician this question, please follow instructions and be patient…remember, it could be your child or grandchild running into traffic to chase a ball and you would want the driver to be at optimal function to apply the brakes!
In our culture, the inability to drive has a significant impact on lifestyle and livelihood. A study published in the Journal of Bone and Joint Surgery, found that 74% of those unable to drive due to injury or surgery are dependent on family and most of the remainder depend on friends. 4% of those unable to drive have no help at all and more than 25% suffer major financial hardship.
The report also found that family physicians, orthopedic surgeons, podiatrists, and physical therapists are keenly aware of this dilemma but often fail to communicate effectively to patients about driving. Most medical professionals express serious concerns about liability regarding return to driving following an injury or surgery. They feel that there is a lack of data to support decisions and inadequate communication among each other. They agree that they must do a better job communicating with patients and their families so they can better prepare for a period of time during their recovery in which they cannot drive.
Recent studies published in the Journal of the American Academy of Orthopaedic Surgeons (JAAOS) and the Journal of Foot and Ankle Surgery (JFAS),determined that there are two significant components in the decision of safely returning to driving after an injury or surgery; the time required for healing and the time required for a return of function. Additionally, it was found that those wearing a surgical shoe or walking boot demonstrated a significantly slower braking response time even in healthy/non-injured individuals wearing the shoe/boot.
During the time required for healing, in addition to the fear of an additional trauma from a motor vehicle accident to the healing body part, there is a general concern about the potential damage that may come from over using the body part to drive before it is adequately healed. For example, a healing fracture in the right lower leg might be compromised or delayed if one must suddenly and forcefully apply the brakes. Also, during this time, it is not unusual for post-injury or post-surgery patients to use pain medications, including narcotics. This will also compromise judgment and reaction time while driving.
Most orthopedic conditions heal in 6 to 8 weeks. However, as many of you may fully know, once a cast or splint is removed, you are not ready to run or jump. Depending on the severity of the injury, it may take many weeks of aggressive physical therapy to regain strength, range-of-motion, agility and dexterity to function at a safe level for a full return to daily activities, including driving.
The current research reinforces the fact that driving safely requires good function of the entire body. For example, just because you broke your shoulder bone but did not fracture your right leg does not mean that you are able to drive safely. Wearing a sling after arm surgery also compromises driving. First, you need a stabilized and healed injury prior to driving. Then, you must work in rehab to make modifications to return to safe driving. Apply the same scenario to injuries or surgery to the spine (neck and lower back).
*Based on research using driving simulators
7 TIPS TO KNOW WHEN YOU ARE READY TO DRIVE:
Remember, every case is unique and there is no substitute for communication with your orthopedic surgeon, podiatrist, family physician and physical therapist.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from patients and sports fans about the nature of the Achilles Tendon rupture injury, recovery, and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to warm-up and exercise during the winter months. A little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears, especially Achilles Tendon rupture. The Achilles tendon is one of the more common tendons torn.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for tendons completely torn, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return to close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
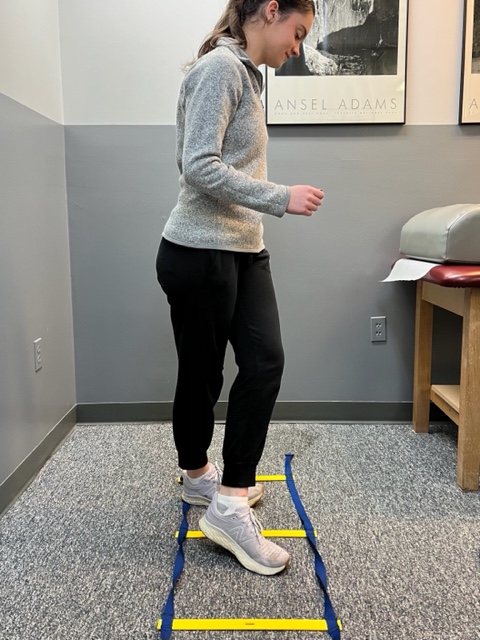
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes: gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity – Photo 1) and proprioceptive and agility drills are essential (Photos 2 & 3).


In PHOTO 1a & 1b: Eccentric Lowering and Lengthening: for the Achillies tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
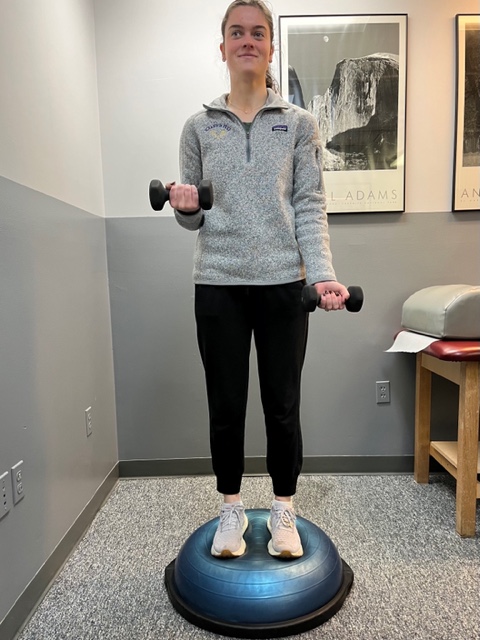
In PHOTO 2: Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
PHOTO 3: Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.
MODEL: Kerry McGrath, student physical therapy aide at Mackarey Physical Therapy
Sources: MayoClinic.com;Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
As most sports enthusiasts know, Aaron Rodgers, former Green Bay Packer quarterback and recent New York Jets QB (for just over a minute and half) suffered a season ending injury when he tore his Achilles tendon in the first game of the 2023/24 NFL season. Since then, I have been answering many questions from many about the nature of the injury and how to prevent it.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to “fit in” a warm-up before running or other activities during the winter months. But, no matter how limited time is, skipping the warm-up is risky. This time of year, one can expect to feel a little cold and stiff, especially if you are over 40, and therefore a little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears. The more commonly torn tendon is the Achilles tendon . Prevention of muscle tears, including the Achilles tendon includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions.
A muscle contracts to move bones and joints in the body. The tendon is the fibrous tissue that attaches muscle to bone. Great force is transmitted across a tendon which, in the lower body, can be more than 5 times your body weight. Often, a tendon can become inflamed, irritated, strained or partially torn from improper mechanics or overuse. Although infrequent, occasionally tendons can also snap or rupture. A tendon is more vulnerable to a rupture for several reasons such as a history of repeated injections of steroids into a tendon and use of medications such as corticosteroids and some antibiotics. Certain diseases such as gout, arthritis, diabetes or hyperparathyroidism can contribute to tendon tears. Also, age, obesity and gender are significant risk factors as middle-aged, overweight males are more susceptible to tendon tears. Poor conditioning, improper warm-up and cold temperatures may also contribute to the problem.
Tendon rupture is very painful and debilitating and must not be left untreated. While conservative management is preferred, surgical management is usually required for complete tears. The purpose of this column is to present the signs, symptoms and management of Achilles tendon ruptures.
The Achilles tendon (also called the calcaneal tendon), is a large, strong cordlike band of fibrous tissue in the back of the ankle. The tendon (also called the heel cord) connects the powerful calf muscle to the heel bone (also called the calcaneus). When the calf muscle contracts, (as when you walk on the ball of your foot), the Achilles tendon is tightened, tension is created at the heel and the foot points down like pushing a gas pedal or walking on tip of your toes. This motion is essential for activities such as walking, running, and jumping. A partial tear of the tendon would make these activities weak and painful, while a full tear through the tendon would render these activities impossible.
With age, the Achilles tendon (and other tendons) gets weak, thin, and dehydrated, thus making it prone to inflammation, degeneration, partial tear or rupture. The middle-aged weekend warrior is at greatest risk. A full or complete tear (Achilles tendon rupture) usually occurs about 2 inches above the heel bone and is associated with a sudden burst of activity followed by a quick stop or a quick start or change in direction, as in tennis, racquet ball, and basketball.
In some instances, the tendon can be injured by a violent contraction of calf when you push off forcefully at the same time the knee is locked straight as in a sudden sprint. Other times, the tendon is injured when a sudden and unexpected force occurs as in a trip off a curb or sudden step into a hole or a quick attempt to break a fall.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog Next Week: Achilles tendon Part II of II.
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
Runners will attempt to conquer 26.2 miles from Forest City to downtown Scranton in the 26th Annual Steamtown Marathon this Sunday. Participants may want to consider new research that suggests the use of compression socks may prevent post race blood clots.
Completing the long and arduous 26.2 mile journey is not an easy task. In fact, the mechanical and physiological toll on your body is tremendous; from painful joints, muscles, tendons, to black and blue toes. Not so obvious, however, is the damage to your deep veins and tissues of the circulatory system. New research indicates that strenuous endurance exercise, such as marathon running, stimulates the clotting mechanisms in your body in response to the multiple micro traumas sustained over 2 or more hours. While most healthy athletes will naturally heal from post exercise clot formation, others may be at risk…those traveling more than 1 hour (by car, bus, train or plane). The risk increases substantially for those with a longer period of travel/sitting post-race, history of previous trauma, blood clots or have the genetic predisposition for clot formation.
Compression socks are familiar to most people as the tight knee-high support stockings worn after a surgical procedure such as a knee or hip replacement to prevent blood clots. They are made with a special fabric and weave design to provide graduated compression (stronger compression at foot and ankle and less at the top of the sock) to promote better circulation and movement of fluids from the foot, ankle and calf back to the upper leg and ultimately the heart. Compression socks work similarly in runners. As the stagnant fluid with lactic acid and other byproducts of exercise is removed from the space, fresh blood, nutrients and oxygen is replaced to foster healing of micro damage to tissue and promote more efficient use of the muscles.
The Journal of Strength and Conditioning Research published a study that found wearing compression socks improved running performance. However, similar studies have failed to support this claim. One finding that has been repeatedly supported in the literature, including The British Journal of Sports Medicine, found that compression socks worn in soccer players and runners improved the rate and magnitude of recovery. Moreover, recent studies, including a study with the Boston Marathon, have demonstrated the reduction in clotting mechanisms in those wearing compression socks AFTER the marathon, as compared with those wearing “sham” socks. Benefits seem to be less obvious for short duration activities or when running 10km or less.
In conclusion, only time will tell if compression socks will improve performance in runners will or be merely a fad based on placebo or true fact supported by scientific research. Based on current wisdom, these socks may offer value and benefit AFTER activities of long duration (more than 1 hour) or long distance running (more than 10km) to expedite the recovery from exercise-induced blood clot formation, muscle soreness from the accumulation of lactic acid and other muscle damage byproducts.
It is this author’s opinion that this product is worth a try. However, whenever you try something new for your sport, trials should occur during practice and if successful used during competition. Consider trying a lower compression to begin (the socks come in different degrees of compression). Even if one is hesitant to use the product while running, it appears the greatest value of the sock is after a prolonged training session or competition to reduce exercise-induced muscle soreness and prevent blood clots, especially in athletes at risk for clotting and those traveling for an hour or more after the race. Additionally, in view of the fact that some studies which showed only minimal to moderate improvement in well-trained athletes, it may be that those in greater need, such as deconditioned individuals attempting to begin a fitness program and novice weekend athletes, may benefit more from compression socks than elite athletes.
TAKE HOME: Runners, cyclists, triathletes, soccer players and others participating in endurance sports should consider compression socks, if not during the activity, certainly following the activity for 24 to 48 hours…especially those at risk for blood clots and those traveling for more than one hour after the race.
Sunday consider trying compression socks and see if they work for you during and more importantly, after your long training runs.
Where to find compression socks:
2XU Compression Racing Sock – www.2XU.com
Scranton Running Company – Olive Street - Scranton
Visit your family doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
Fall is here, cross-country running season has begun and the 26th Steamtown Marathon is only a few weeks away! With that in mind, running injuries, some very specific to women, are on the increase…
While driving to or from work have you noticed more local running enthusiasts in the past few years? Moreover, have your noticed that most of the runners are women? Scranton Running Company has contributed to NEPA’s participation in a national trend; more women are engaged in running than men! Female runners account for 9.7 million runners (57%) while 7 million males run on a national level.
With this surge, the female runner has been subjected to a host of related injuries, including shin splints, which often lead to stress fractures. New research has found that stress fractures may be related to the loss of weight and body mass associated with the sport.
A recent study from Ohio State University found that female runners with a Body Mass Index (BMI) below 19 may have a higher risk of developing stress fractures than women with a BMI of 19 or above. Furthermore, the study also found that these women took longer to recover from these injuries.
According to Timothy Miller, MD, “When body mass index is very low and muscle mass is depleted, there is nowhere for the shock of running to be absorbed other than directly into the bones. Until some muscle mass is developed and BMI is optimized, runners remain at increased risk of developing a stress fracture,”
The study also found that female runners with a BMI of 19 or higher with severe stress fractures required 13 weeks to recover from their injuries and return to running. Runners with a BMI lower than 19, however, took more than 17 weeks to recover.
They concluded that women should know their BMI and consult with a medical professional to maintain a healthy number. Additionally, women should cross-train and include resistance training to improve the strength and muscle mass of the lower extremities to prevent injury.
The current BMI wisdom, according to the National Institutes of Health, is 19.8 for men and 24 for women, however, strong and competitive women tend to have a BMI of 26. A BMI of 18 is considered malnourished.
Body mass index (BMI) is a measure of body fat based on height and weight of adult men and women over 20 years of age, according to the National Institutes of Health.
BMI = (weight in pounds / height in inches squared) X 703)
Example 1: a person who weighs150 pounds and is 68 inches (5 feet 8 inches) tall has a BMI of 22.8
Example 2: a person who weighs 110 pounds and is 66 inches (5 feet 5 inches) tall has a BMI of 17.7
Underweight < 18.5%
Normal weight 18.5 to 24.9%
Overweight 25 to 29.9%
Obesity 30 and over
A stress fracture is fatigue damage to bone with partial or complete disruption of the cortex of the bone from repetitive loading. While standard x-rays may not reveal the problem, a bone scan, and MRI will. It usually occurs in the long bones of the leg, mostly the tibia (shin bone) but also the femur (thigh) and foot. Occasionally, it occurs in the arm.
FEMALE RUNNERS WITH BMI LOWER THAN 19 – is a primary risk factor.
10-21% of all competitive athletes are at risk for stress fractures. Track, cross country and military recruits are at greatest risk. Females are twice as likely as males to have a stress fracture. Other athletes at risk are: sprinters, soccer and basketball players, jumpers, ballet dancers are at risk in the leg and foot. Gymnasts are also vulnerable in the spine while rowers, baseball pitchers, golfers and tennis players can experience the fracture with much less frequency in the ribs & arm.
The problem is much more prevalent in weight bearing repetitive, loading sports in which leanness is emphasized (ballet, cheerleading) or provides an advantage (distance running, gymnastics).
Stress fractures usually begin with a manageable, poorly localized pain with or immediately after activity such as a shin splint. Over time, pain becomes more localized and tender during activity and then progresses to pain with daily activity and at rest.
Source: Ohio State University, Science Daily
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy!
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Paul's Articles, visit our exercise forum!
