Spring is just around the corner so it is time for running enthusiasts to lace up their sneakers, get outside and run! Runners are addicted to running for good reason. There is nothing like it! No exercise offers so much in such little time. For example, the caloric expenditure while running is higher than for most other exercises, including biking. Also, it allows for fresh air and beautiful scenery with a minimal investment in clothing or equipment. It requires little skill and time to learn. Runners suffer from less depression, colds and flu symptoms, and experience less pain due to an endorphine release (natural chemical in the brain associated with euphoria and pain control) that is greater than found in other sports and activities. These are some of the motives that cause people to run every day, in spite of the constant loading and wear and tear on the joints.
To be a competitive runner and have longevity in the sport, optimal form is necessary. Moreover, a recent study shows that a runner can decrease the stresses on the lower body and reduce the incidence of stress fractures when trained to run with proper form using visual feedback while on a treadmill. The application of this information has significant implications for training programs for runners for the prevention and recovery from injury. One such low impact method is called the “Pose Running Technique,” by Dr. Nicholas Romanov. It is a “soft landing” method which promotes; an S-like body position with slightly bent knees, a slightly forward lean at the ankles to employ gravity and momentum, lifting the feet up under the hips, and landing on the ball of the foot under the body to absorb the center of mass.
It is my opinion, that the best runners, with the least injuries, such as Jordan Hoyt, speedster from Abington Heights, employ these techniques naturally. Additionally, many of the world’s best runners use coaches and trainers to assist them in their quest for success and injury prevention by using perfect form. However, for the rest of us, we must learn to maximize the efficient use of the body as it works with, not against gravity. We must learn to run “soft” to prevent injuries.
A slight upward tilt of the head to allow a view of the horizon ahead should be most comfortable. Avoid looking down or up to extremes. Do not rock or rotate the head while running.
Loose and relaxed shoulders set the tone for a good run. Keep them level without tilting side to side or rotating left to right. Avoid holding the shoulders in a tight and high position.
Loose and relaxed arms also set the tone for a good run. A good arm swing is always in forward motion in a linear direction and stays between the waist and lower chest. Never clench the fist. Do not rotate or twist the arms across the body.
If the head, shoulders and arms are in correct position, then the torso will be upright. An erect running posture is necessary to promote efficient movement and breathing. The posture that you assume when taking a deep breath is the correct torso position for good breathing while running.
The hips will follow the position of the parts above in a linear forward direction. However, if the torso leans forward because the head hangs down then the hips will tilt downward. If the arms swing and torso rotates side to side, then the hips will also rotate.
Sprinters need to lift the knees high to thrust the lower legs forward. Long distance runners cannot maintain a high knee lift for a long period of time, however, a slight knee lift with a shorter but quicker stride is more efficient. Proper running requires the foot to softly strike the ground with the knee slightly bent. If the knee is fully extended in front of the body upon impact, the stride is too long and the force too great.
To excel as a runner, when the foot hits the ground it should land lightly, between the heel and the midfoot. The ankle is flexed and rolls quickly forward to the toes to push off the ground with maximum force. The calf muscle propels the runner forward. Efficient running has a quiet and springy landing. A loud foot slap on impact is a sign of poor form and results in excessive force transferred to the lower leg. The foot should spend as little time as possible in contact with the ground…thus a soft runner “floats” when they run.
SOURCES: Runner’s World, Pose Running Technique (www.posetech.com), Journal of Orthopaedic and Sports Physical Therapy.

NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
Pre-pandemic we saw increased popularity of local races such as the Steamtown Marathon and Scranton 1/2 Marathon. With that, local interest in running was exploding and will hopefully return to normal soon. However, during the pandemic, especially when fitness centers were closed, many took seasoned and beginner runners to the streets to improve fitness and alleviate stress. However, as a health care provider, I am seeing a significant number of first time runners visit my office with a wide variety of injuries that are very preventable with a modicum of good judgment.
Runners are addicted to running for good reason. There is nothing like it! No exercise offers so much in such little time. Caloric expenditure is higher than in most other exercises, including biking. Running also allows for fresh air, beautiful scenery, minimal investment in clothing or equipment, little skill and time to learn. Moreover, the benefits are many; runners suffer from less depression, colds and flu symptoms, and experience less pain due to an endorphin release (a natural chemical in the brain associated with euphoria and pain control.)
This column will be dedicated to those who are interested in beginning a running program for all the reasons mentioned above and more. The program is designed to promote a safe and gradual introduction or return to running as form of exercise. The initial goal is to help you attain 30 minutes (approximately 2 miles) of running at a slow, relaxed and safe pace. This 30 minute goal is the standard used in most research that shows improvement in weight control, cholesterol, heart disease, blood pressure and adult onset diabetes. The 8 week program is a simple and safe program that begins with more walking than running and gradually reverses the proportion. The first two miles are the hardest and once mastered; one can begin to build on mileage and intensity if desired. For those interested in advancing to a half or full marathon, I recommend the book “The Marathon” by Jeff Galloway who advocates a run/walk program as you increase distances. Visit his website at: www.jeffgalloway.com.
The appearance of an arch in a weight bearing position does not automatically exclude the individual from excessive supination or pronation. Consult a podiatrist or an orthopedic physical therapist to determine the propensity toward supination, pronation or neutrality of the foot and ankle.
Note: New Balance, Brooks, Asics, Mizuno & Saucony all make quality running shoes to accommodate a supinated, pronated or normal foot.
Mon.Wed.Fri.Sat: Run 1 minute. Walk 2 minutes. Repeat 10 Times
Tues.Thurs: Walk 30 minutes
Sun: Rest
Mon.Wed: Run 2 minutes. Walk 1 minute. Repeat 10 Times
Fri.Sat: Run 3-4 minutes. Walk 1 minute. Repeat 6-7 Times
Tues.Thurs: Walk 30 minutes
Sun: Rest
Mon.Wed: Run 5 minutes. Walk 1 minute. Repeat 5 Times
Fri.Sat: Run 6 minutes. Walk 1 minute. Repeat 4 Times
Tues.Thurs: Walk 30 minutes
Sun: Rest
Mon.Wed: Run 8 minutes. Walk 1 minute. Repeat 3 Times THEN: Run 3 minutes
Fri.Sat: Run 10 minutes. Walk 1 minute. Repeat 2 Times THEN: Run 8 minutes
Tues.Thurs: Walk 30 minutes
Sun Rest
Mon.Wed: Run 12-13 minutes. Walk 1 minute. Repeat 2 Times THEN: Run 2-4 minutes
Fri.Sat: Run 14-15 minutes. Walk 1 minute. Repeat 2 Times THEN: Run 2 minutes
Tues.Thurs: Walk 30 minutes
Sun: Rest
Mon.Wed: Run 16-17 minutes. Walk 1 minute. THEN: Run 12-13 minutes
Fri.Sat: Run 18-19 minutes. Walk 1 minute. THEN: Run 10-11 minutes
Tues.Thurs: Walk 30 minutes
Sun: Rest
Mon.Tues.Wed: Run 20-22 minutes. Walk 1 minute. THEN: Run 7-9 minutes
Fri.Sat: Run 24-26 minutes. Walk 1 minute. THEN: Run 3-5 minutes
Thurs: Walk 30 minutes
Sun: Rest
Mon.Tues.Wed: Run 27-28 minutes. Walk 1 minute. THEN: Run 1-2 minutes
Fri.Sat: Run 29-30 minutes. Walk 1 minute. THEN: Run 0-1 minutes
Thurs: Walk 30 minutes
Sun: Rest
SOURCE: Runner’s World
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” NEXT WEEK…RUN WITH GOOD FORM!
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
Injuries due to falling are a very common problem in the elderly. Hip fractures are the most common injury due to falling in the seniors. According to the American Academy of Orthopaedic Surgeons, each year more than 300,000 people are hospitalized for hip fractures in the United States. These fractures represent 72% of all fracture costs, totaling more than 12 billion dollars in 2005 and, not surprisingly, 90% occurred in those 65 and older. Most hip fracture patients who previously lived independently will require family assistance, home or long term care and 50% will require a cane or walker.
A recent study by the American Physical Therapy Association found that patients benefited from a physical therapy evaluation to determine their risk level for falling. If a high-risk level is found on a falls assessment, physical therapy interventions can be successfully employed to improve strength, balance, and coordination and falls prevention. Also, a well-balanced diet, exercise, Calcium with vitamin D supplements and medications can help prevent or retard osteoporosis and prevent hip fractures.
***Always perform slowly, alternate right and left sides, limit other distractions and concentrate on the exercise to retrain the brain, 10-20 times each 2-3 times per day.
***Caution: Do not do standing exercises without assistance or supervision if needed
Face a countertop and hold onto it with both hands. Hike your hip and knee up to 90 degrees as if you are marching. Hold the position for 3-5 seconds on one leg and lower slowly. Repeat this on the other leg and alternate 10 times.

Face a countertop and hold onto it with both hands. Lift your leg up 30 degrees as if you are spreading your legs apart. Hold the position for 3-5 seconds on one leg and lower slowly to cross over the middle. Repeat this on the other leg and alternate 10 times.
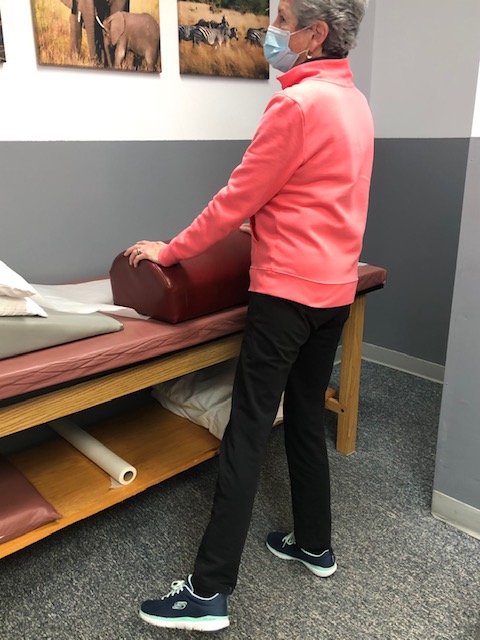
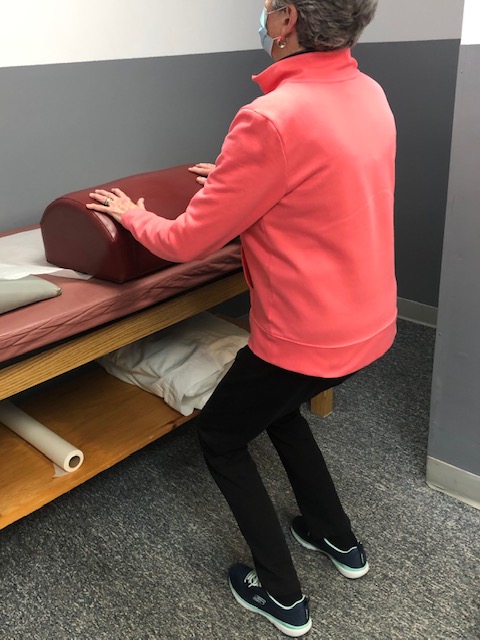
Face a countertop and hold onto it with both hands. Bend your hip and knee down to 45 degrees to a squatting position. Hold the position for 3-5 seconds on both legs and return to standing slowly. Repeat this 10 times. Once strong enough try on one leg at a time and alternate.
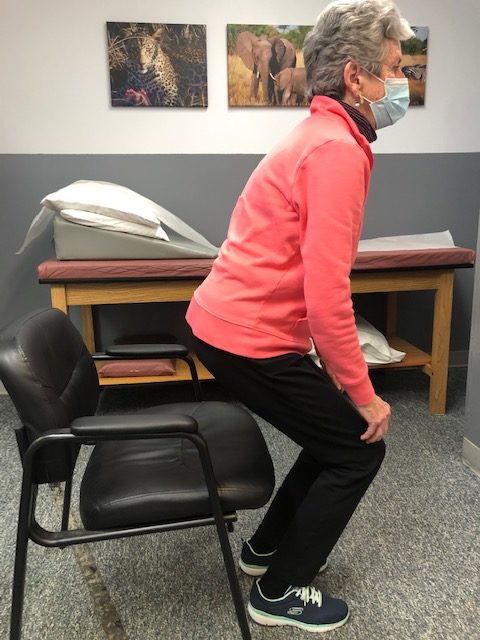
Sit in a chair with arm rests. Get out of chair only using your legs. Hold the position for 3-5 seconds and return to sitting. If necessary, use 1 or 2 arms to assist. Repeat this 10 times. Focus on trunk core stabilization and leg strength. Use more leg muscles and less arm muscles as strength improves.
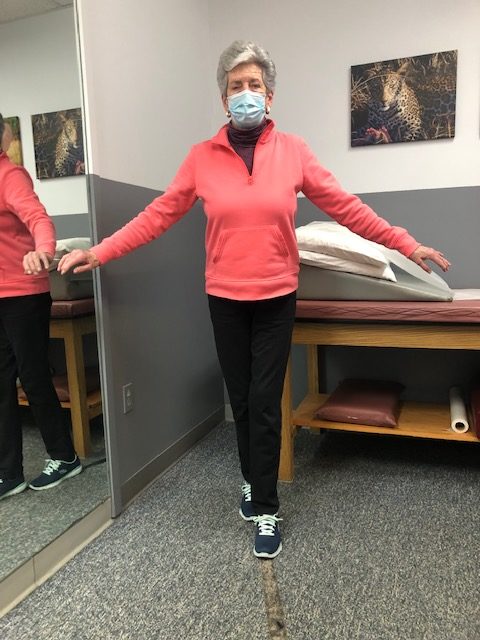
Place a straight line on the floor and practice “walking the line” with the right then left foot on the line.
Hold onto a chair while bending one knee and shifting your weight to the other leg. Hold for 3-5 seconds and repeat with the other leg. Increase time 10 -15 -20 seconds as tolerated.

If you feel you or a loved one may be at risk for falling or a hip fracture, ask your family physician if a physical therapy consultation for a falls prevention program to prevent hip fractures may benefit you.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit www.mackareyphysicaltherapy.com/forum
When an older loved one sustains a serious injury it is traumatic for the entire family and mine is no exception. My grandmother and father enjoyed 90 wonderfully active years; however, their independence was lost the same way more than one-third of a million people lose their independence each year… hip fractures! As a doctor of orthopedic physical therapy, I feel remise that I could not prevent this from happening. What most of us fail to realize is that his fracture, like many, was more than just an orthopedic problem …it involves age, gender, diet, exercise, vision, leg strength, medications, environmental risks, and vestibular problems (inner ear problems effecting balance).
Injuries due to falling are a very common problem in the elderly. Hip fractures are the most common injury due to falling in the seniors. According to the American Academy of Orthopaedic Surgeons, each year more than 300,000 people are hospitalized for hip fractures in the United States. These fractures represent 72% of all fracture costs, totaling more than 12 billion dollars in 2005 and, not surprisingly, 90% occurred in those 65 and older. Most hip fracture patients who previously lived independently will require family assistance, home or long term care and 50% will require a cane or walker.
Several risk factors for hip fractures have been identified. While some factors are somewhat controllable and may improve bone quality, (diet, exercise, smoking, alcohol) others are not.
Vestibular or inner ear problems
Preventing a fall can not only save your independence but also your life! Preventing injuries from falls reduces the need for nursing home placement.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Hip Fractures - Part II of II
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's Articles visit: www.mackareyphysicaltherapy.com/forum
More than 65 million people, almost 30% of the population in the United States, are actively involved in providing 20 or more hours of care for a chronically ill, disabled, or aged family member or friend each week. As our population continues to age, this number is expected to grow rapidly.
The role of a caregiver is multifaceted and often involves tasks and skills beyond the education or comfort level of most providers. Some examples include; managing money, paying bills, shopping, cleaning, maintaining and repairing a home, dispensing and injecting medications, cleaning wounds, changing dressings, catheter management, bed baths, assisting in position changes, transferring from the bed to the chair, ambulation, stair climbing, bathroom assistance for toileting and showering and many other responsibilities. Consequently, a caregiver is often at risk for mental, spiritual and physical fatigue or breakdown. It is no surprise that depression, illness and injury often plague a caregiver and eventually, the caregiver is in need of a caregiver. One of the most common injuries suffered by a caregiver is back pain.
Lower back pain (LBP) is one of the most common problems in our society. Over 90% of all Americans will suffer from it at least once in their lives. It is generally agreed that prevention is the best treatment for LBP.
As little as 10 extra pounds puts great stress on your lower back. It also makes it more difficult to maintain good posture. Eat well and exercise regularly.
Aerobic exercise will help prevent weight gain and stiffness for a healthier lower back. It will also help with the stress and depression associated with providing care for a loved one. Perform mild aerobic exercise such as walking 3-5 times per week for 30-45 minutes. You can also use an elliptical or bike at home while your loved one is resting. Get outdoors and take multiple short walks …go around the block a few times per day.
Core stabilization exercises designed to strengthen the abdominal and lower back muscles will help prevent injury. Some examples of core exercises are:
Pelvic Tilt - lying on your back and performing a pelvic tilt as you flatten you lower back into the floor.
Pelvic Tilt and Heel Slide - lying on your back, hold a pelvic tilt as you slide your one heel up and down and repeat with the other heel.
Core on Ball - Perform arm exercises such as biceps and triceps with light weight while sitting on a therapeutic ball while simultaneously trying to hold an isometric contraction of your abdominal and lower back muscles.
Smoking effects natural healing because it constricts the small blood vessels. Smokers have a much higher incidence of LBP and failure from lower back surgery.
Good posture is critical for a healthy back. When sitting, standing or walking maintain a slight arch in your lower back, keep shoulders back, and head over your shoulders. In sitting, use a towel roll or small pillow in the small of the back.
Caregivers spend much of the day with their spine bent over a bed or chair feeding, bathing, and lifting a loved one. Postural exercises are designed to stretch your back in the opposite direction of this forward flexed position. Examples include:
Bend your knees, maintain an arch in the back with head up, and bend over as little as possible. Bend the knees of your loved one; roll their trunk toward you to get their legs over the edge of the bed as you pivot their weight on their butt to get them sitting upright.
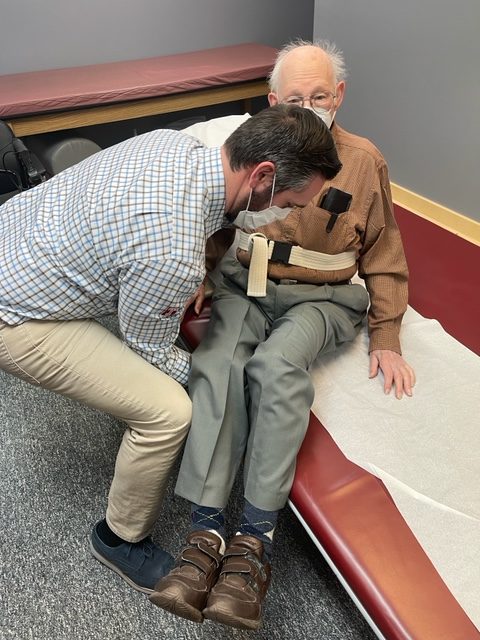
Bend your knees, maintain an arch in the back with head up, and bend over as little as possible. Place your hands around the waist or on a transfer belt. Use your legs, turn with feet, and do not twist spine. Block the feet and knees of your loved-one with your feet and knees and use them to pivot and transfer from the bed to the chair. Be sure the chair is along side of the bed and arm of chair removed if possible before the lift.
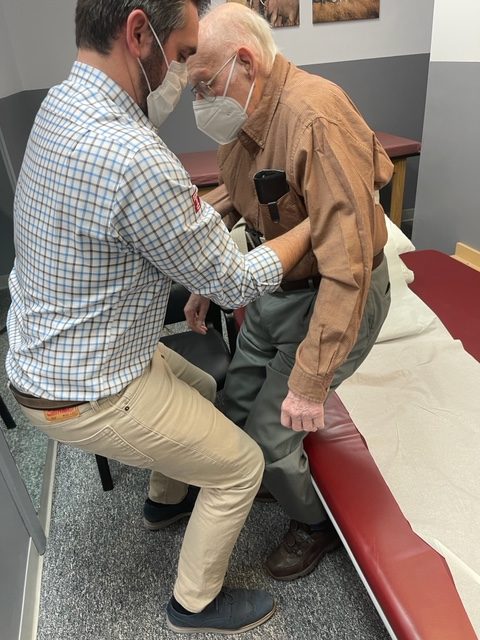
Transfer Belt - Use a transfer belt around the waist of the patient. Grip the transfer belt, instead of the patient or clothing, during the lift or when ambulating. Lower Back Lifting Belt - Also, if you have a back problem, consider using a lifting belt or back brace to protect your back when lifting the patient. Immediately following the lift, stand up straight and stretch lower back into extension.
Transfer belts and lower back lifting belts can be found online or at your local pharmacy.
Lift Chair – For patients that require maximum or moderate assistance and only one caregiver is available to lift or transfer, an electric lift chair should be considered.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at GCSOM.
Visit your doctor regularly and listen to your body.
For all of Dr. Mackarey's articles visit: https://mackareyphysicaltherapy.com/forum/
I am sure that many of you feel as I do…it is hard to believe that I am living in the year two thousand and TWENTY-TWO! Moreover, I hope you share my sentiments that each year, despite the trials and challenges of the pandemic, each month, week, day, and minute is a gift, not to be taken for granted. And that is why we resolve at this time each year to make a concerted effort to improve ourselves; mentally, physically and spiritually, so that we may live a longer and healthier life, in order to spend more time with the friends and family we love.
Not surprisingly, getting physically fit and losing weight are the top resolutions to begin each New Year. According to the University of Pittsburgh Medical Center, 10 million Americans choose to join one of the 45,000 health clubs and hope to get fit and healthy for life (in non pandemic years). Unfortunately, if starting an exercise program is the hard part, than sticking to it is the hardest part. And, with the Omicron surge limiting access to indoor gyms and fitness centers, compliance may be even more challenging this year.
Once the initial excitement and enthusiasm wears off, so too does the discipline and determination necessary to overcome the many distractions in our lives to make exercise a priority for life. Diane Klein, PhD polled long-term exercisers (those exercising at least 3 times per week for more than 13 years) what motivated them to “stick with the program.” The answers are in order of importance. Please note that “appearance” was NOT at the top of the list.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit: mackareyphysicaltherapy.com
You are never too old to exercise! This is the second of two columns dedicated to appropriate exercise for the elderly. Last week I discussed basic strengthening exercises. This column will address three additional components necessary for independence in the elderly: flexibility, balance and endurance. While it may not be as valuable for those fortunate to be over 75 years of age and capable of running, skiing and playing tennis, you may still find a noteworthy pearl of wisdom.
Why would someone 75 or 80 be interested in a basic exercise program? Well, one must maintain adequate flexibility, strength, balance and endurance to safely function in daily activities around the house. For example, the most common goals of elderly patients are: climbing stairs, getting in and out of a shower, putting on shoes and socks, tucking in a shirt or fastening a bra, cooking, cleaning, and carrying groceries or laundry.
Remember, for most people it is more harmful not to exercise, so contact you physician to discuss whether independent exercise is appropriate for you. You may need to consult with a physical therapist to get started.
Flexibility Exercises involve moving the arms, legs and trunk through comfortable range of motion to give you more mobility in order to improve your ability to perform daily activities such as tucking in a shirt, tying shoes or fastening a bra. Best if performed after strength exercises because the muscles and joints will be warm and limber. Always perform slowly with slight stretch sensation and no pain. No bouncing or over stretching!
These exercises are to be performed while sitting in a chair with a backrest, slowly, 5 repetitions, 3-5 times per week.
Balance Exercises involve strengthening muscles that keep the body upright and stable in standing in order to improve your ability to perform daily activities without falling. According to the NIH, 300,000 US hospital admissions for broken hips occur each year due to falls. Check with your physician if you have a history of dizziness before performing these exercises on your own. Best if performed with someone at home or some assistance. Always use a countertop or back of chair to hold onto for support.
Endurance Exercises involve any activity such as walking, swimming, biking or raking leaves that elevates your heart rate and breathing for an extended period of time. Check with your physician if you have a history of heart problems or dizziness before performing these exercises on your own. Best if performed with someone at home or some assistance. Start off slowly for only 5 minutes and add 1-2 minutes each week or 2. Wear good and comfortable shoes – no heels!
While not all of these endurance exercises may be appropriate for you, one or two of these may offer a good starting point.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate profession of clinical medicine at Geisinger Commonwealth School of Medicine.
For all of Dr. Mackarey's articles visit mackareyphysicaltherapy.com
You are never too old to exercise! A reader who described herself as “elderly” asked me if she was too old to exercise. Without knowing her age, I replied that she was not. I did qualify my response with the fact that exercise must be adjusted to meet the individual needs of a person based on age, health status and goals. Her question, however, led me to think of the many “elderly” who may be apprehensive to begin an exercise program for a variety of reasons. Fear of injury and lack of information may be two reasons. Another reason, according to this inquiry, is the fact that so many exercise programs featured in the media are geared to the young and healthy or baby boomers and few focuses on the needs of those over 75, home bound and weakened by age and inactivity. Those running, biking, skiing, golfing at 75 and over and do not fall into this category, please do not be offended, you are the exception. God bless you!
Why would someone 75 or 80 be interested in an exercise program? Well, one must maintain adequate flexibility, strength, balance and endurance to safely function in daily activities around the house. For example, the most common goals of elderly patients are: climbing stairs, getting in and out of a shower, putting on shoes and socks, walking safely for functional distances, tucking in a shirt or fastening a bra, cooking, cleaning, and carrying groceries or laundry.
The National Institute of Health (NIH) recommends four areas of concentration for elderly persons to concentrate on in order to maintain safety and independence: strength, flexibility, balance and endurance. It will be the purpose of this column to recommend safe, practical and easy exercises that focus on each of these categories.
Remember, for most people it is more harmful not to exercise, so contact your physician to discuss whether independent exercise is appropriate for you. You may need to consult with a physical therapist to get started.
Strength Exercises involve using the muscles to move the arms and legs against resistance such as a weighted object, dumbbells, resistance bands, and body weight against gravity. Strength is necessary to perform daily activities such as walking, lifting a ½ gallon of milk, transferring to a shower or chair safely.
These exercises are performed while sitting in a chair with backrest, slowly, 5 -10 repetitions, and 3-5 times per week. No weight is used in the beginning, only the weight of the arm against gravity. In 1-2 weeks a light 1-2 pound weight and light resistance band may be added.
Once you have mastered these exercises against gravity, then advance to using light weights or light resistance bands. Ankle weights are very inexpensive and can be purchased in 1 pound increments. Light resistance bands are available in yellow and red in colors.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week: Never To Old To Exercise – Part II of II
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate profession of clinical medicine at Geisinger Commonwealth School of Medicine.
For all of Dr. Mackarey's articles visit http://mackareyphysicaltherapy.com/forum
The body is beautifully designed to constantly change and make adjustments to maintain homeostasis...a healthy place where all systems work together in perfect equilibrium. However, when things are not working as planned, your body is also designed to give you feedback. Sometimes the feedback is benign (like a stomach ache from eating too much), while other times the feedback is important and should not be ignored (like severe lower right-sided abdominal pain that makes you nauseous or vomit). When calling your physician or reporting to the emergency department with a problem, try to be clear and concise (when symptoms began, the degree of pain from 1 to 10, and bring a medication and allergy list with your medical history).
While chest pain can be from many benign causes such as a pulled muscle from heavy lifting it can also be more serious. A dull ache, sharp stabbing pain, crushing or burning sensation, especially when associated with radiating pain to the neck, jaw and left shoulder can be a sign of a heart attack and should not be ignored. If the symptoms fail to subside after 5 minutes of rest, call 911 or have someone take you to the closest emergency department.
Sudden slurred speech and or blurred vision often associated with weakness in an arm or leg can be a sign of a stroke. These signs can also be associated with intoxication from alcohol or drugs. Call 911 or have someone take you to the closest emergency department.
Abdominal pain can occur for many non emergency reasons; constipation, gas, overeating, stress or muscle strain. However, if the pain is associated with nausea, fever, bloody stools, difficulty breathing, and vomiting blood, than it may be related to a much more serious problem such as appendicitis. Other causes include: irritable bowel syndrome, gastrointestinal disease, gastritis, or hernia. Consult your physician immediately or get to an emergency department.
Losing weight is the most common health and wellness goal. However, when weight loss of 10 or more pounds in 4 to 6 months is not associated with conscious dieting, it may be a sign of a much more serious problem...consult your doctor.
According to the Mayo Clinic, an unexplained drop in weight could be caused by various conditions —including overactive thyroid (hyperthyroidism), diabetes, depression, liver disease, cancer or disorders that interfere with how your body absorbs nutrients (malabsorption disorders).
A fever is often a normal response when your body is fighting infection and usually not a cause for alarm. However, persistent fever can signal a hidden infection, which could be anything from a urinary tract infection to tuberculosis. In some cases, cancerous (malignant) conditions, such as lymphomas , cause prolonged or persistent fevers, as can some medications.Call your doctor if your temperature is 103 F (39.4 C) or higher or you've had a fever for more than three days.
There are many non-serious reasons for shortness of breath such as; very strenuous exercise, extreme temperatures, massive obesity and high altitude all can cause shortness of breath. However, it can also be a sign of a medical problem. If you have unexplained shortness of breath, especially if it comes on suddenly and is severe, seek emergency medical care.
Mayo Clinic lists the following medical causes for breathlessness: chronic obstructive pulmonary disease, bronchitis, asthma, pneumonia, a blood clot in the lung (pulmonary embolism), as well as other heart and lung problems. Difficulty breathing can also occur with a panic attack — a sudden episode of intense anxiety that triggers severe physical reactions when there is no real danger or apparent cause.
Consult your doctor if you notice unusual or unexplained changes in your stool (relative to what is normal for you). Some serious signs are: bloody, black or tarry-colored stools, persistent diarrhea or constipation, and unexplained urges to have a bowel movement.
Changes in bowel habits could signal a bacterial, viral or parasitic infection. Other possible causes include irritable bowel disease and colon cancer.
Confusion and personality changes could be caused by many problems, including infection, poor nutrition, mental health conditions or medications. However, seek medical attention if you have sudden: poor thinking skills, difficulty focusing, sustaining or shifting attention, or behavior changes.
If you notice that you consistently have a sensation of fullness in your stomach, even though you have been eating less than usual, get checked by your doctor. This sensation is called early satiety. Early satiety can be associated with nausea, vomiting, bloating or weight loss. Experts at the Mayo Clinic recommend that you consult with your doctor about the possible causes of early satiety including; gastroesophageal reflux disease, commonly known as GERD, and peptic ulcers. In some cases, a more serious problem, such as pancreatic cancer, could be a factor.
If you see very bright and sudden flashes of light or bright spots it could be a sign of a serious problem with your eyes. While these symptoms are often associated with severe migraines, it can also be a sign of a more serious eye problem called a detached retina. If so, it requires immediate medical care can help prevent permanent vision loss.
Sources: Mayo Clinic, NIH – National Institute on Aging
Read Dr. Mackarey’s Health & Exercise Forum – Every Monday
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit: mackareyphysicaltherapy.com
The number one resolution each year is to lose weight. The internet is flooded with endless recommendations for diet and exercise. While not guaranteed, the recommendations below are safe, simple and easily implemented. And, it is a good way to start your day…give it a try!
Source: WebMD, Mayo Clinic
Read Dr. Mackarey’s Health & Exercise Forum – Every Monday
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles visit: mackareyphysicaltherapy
