Last week in Health & Exercise Forum, we discussed dehydration as a potentially life-threatening problem, especially in those over 60. Summer heat and humidity are here and the risk of heat related illnesses are greater than normal. Age, diet, illness and medications are some of the many reasons why elders suffer from dehydration not only in the summer heat, but year round. Furthermore, age related changes in 50-60 year olds can also make one vulnerable to dehydration, especially if they are active and exercise in the heat.
It is widely accepted that the best treatment for dehydration is prevention. One must take a proactive approach to ensure and/or encourage adequate fluid intake, especially with age and in high temperatures. Consider some of the following practical tips to promote optimal hydration.
Remember, knowledge and awareness of the symptoms of and the prevention of dehydration can reduce unnecessary hospitalizations and maximize health and well-being for the elderly and not-so-elderly individual.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
Contributor: Janet M. Caputo, DPT, OCS

NEXT MONDAY! – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, check out our exercise forum!
Summer heat and humidity are here and the risk of heat related illnesses are particularly high for those over 65, especially dehydration. Age, diet, illness and medications are some of the many reasons why elders suffer from dehydration not only in the summer heat, but year round. Furthermore, age related changes in 50-60 year olds can also make one vulnerable to dehydration if they are active and exercise in the heat. Not long ago, a local medical professional and good friend of mine was hospitalized for several days due to dehydration and associated illness. He is an active, fit, healthy 59 year old who continued his daily running for exercise during the June/July heat wave.
It is often forgotten that, next to oxygen, water is the nutrient most needed for life. A person can live without food for a month, but most can survive only three to four days without water. Even though proper hydration is essential for health, water gets overlooked as one of the six basic nutrients. Dehydration occurs when the amount of water taken into the body is less than the amount that is being lost. Dehydration can happen very rapidly (i.e. in less than eight hours); the consequences can be life threatening and the symptoms can be alarmingly swift.
In the body, water is needed to regulate body temperature, carry nutrients, remove toxins and waste materials, and provide the medium in which all cellular chemical reactions take place. Fluid balance is vital for body functions. A significant decrease in the total amount of body fluids leads to dehydration. Fluids can be lost through the urine, skin, or lungs. Along with fluids, essential electrolytes, such as sodium and potassium, are also perilously depleted in a dehydrated individual.
Dehydration is the most common fluid and electrolyte disorder of frail elders, both in long term care facilities and in the community! Elders aged 85 to 99 years are six times more likely to be hospitalized for dehydration than those aged 65 to 69 years. More than 18% of those hospitalized for dehydration will die within 30 days, and associated mortality increases with age. Men appear to dehydrate more often than women and dehydration is often masked by other conditions.
Elderly individuals are at heightened risk for dehydration for several reasons. Compared to younger individuals, their regulatory system (i.e. kidneys and hormones) does not work as well and their bodies have lower water contents. The elderly often have a depressed thirst drive due to a decrease in a particular hormone. They do not feel thirsty when they are dehydrated. This is especially true in hot, humid weather, when they have a fever, are taking medications, or have vomiting or diarrhea. They have decreased taste, smell, and appetite which contribute to the muted perception of thirst. Because of dementia, depression, visual deficits, or motor impairments, elderly persons may have difficulty getting fluids for themselves. Many elderly individuals limit their fluid intake in the belief that they will prevent incontinence and decrease the number of trips to the bathroom. The medications that they are taking (e.g. diuretics, laxatives, hypnotics) contribute to dehydration.
Elders may suffer headaches, fainting, disorientation, nausea, a seizure, a stroke, or a heart attack as a result of dehydration. The minimum daily requirement to avoid dehydration is between 1,500 (6.34 cups) and 2,000 ml of fluid intake per day. Six to eight good-sized glasses of water a day should provide this amount. Better hydration improves well-being and medications work more effectively when an individual is properly hydrated. Those who care for the elderly whether at home or in a health care facility need to be alert to the following symptoms (but these symptoms apply to both young and old):
Plain old tap water is a good way to replenish fluid loss. Some energy drinks not only have excess and unneeded calories but also contain sugar that slows down the rate at which water can be absorbed form the stomach. Consuming alcoholic and caffeinated beverages actually has an opposite, diuretic effect!
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
Contibutor: Janet M. Caputo, DPT, OCS
NEXT MONDAY! – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next week: Part II - Dehydration Prevention”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, check out our exercise forum!
It is time to celebrate the 4TH of July with some fun in the sun…but don’t forget to protect your skin! A little awareness and some precautions can go a long way to make this holiday weekend safer!
Despite the fact that we have limited exposure to sunny days in NEPA (50%), skin cancer still exists in large numbers. Skin cancer is the most common cause of cancer in the United States. While there are several types of skin cancer and not necessarily all are deadly, procedures to remove these skin cancers are both costly and frequently result in unsightly scars. The most dangerous type of skin cancer, called melanoma, results in an estimated 10,000 deaths per year. The good news? Nearly all skin cancers are preventable!
The majority of skin cancers are caused by harmful ultraviolet (UV) rays from the sun. Two major types are UVA and UVB:
In the field of anti-aging, advertisers make lofty promises for many products that claim to contain or boost collagen. Whether or not these work is a whole other discussion, but what is collagen and what does it have to do with wrinkles?
Collagen is the most abundant protein in the human body. It is found in nearly all tissues and organs, and plays a crucial role in maintaining structural integrity. Unfortunately, collagen production naturally decreases with age. This causes many of the findings we associate with older age, such as sagging skin and wrinkles, as well as joint pain. Collagen also works together with another important protein called elastin, which helps to maintain elasticity – a feature commonly associated with youthful skin.
When exposed to UV rays, these proteins can become damaged. For instance, studies have shown that skin exposed to UV rays increases the expression of proteins called matrix metalloproteinases, or MMPs. You can think of these MMPs as collagen’s enemy, as they cause their degradation. This results in a decrease in collagen’s structural function leading to loose and wrinkled skin. UV rays can also stimulate the production of reactive oxygen species. These are substances such as hydrogen peroxide and bleach, which further cause destruction of skin’s microscopic structure.
So, you’re convinced and have decided to keep your skin healthy and youthful – what next? With so many different products on the market, choosing a daily sunscreen can become a difficult task. Here are a few pointers:
Another consideration when choosing a sunscreen is chemical versus physical blockers:
If preventing skin cancer isn’t incentive enough to wear sunscreen daily and avoid excessive sun exposure (and indoor tanning booths!), then consider the rapid effects on aging the sun’s rays can have. While a tan may look good for a week, avoiding exposure to UV rays will both delay and prevent aging for years.
For more information on skin cancer and prevention, please visit the Center for Disease Control’s website (https://www.cdc.gov/cancer/skin/) and contact your physician for specific concerns regarding spots on your skin.
Guest Contributor: Eduardo Ortiz, MD, Geisinger Commonwealth School of Medicine 2018
NEXT WEEK! Read Dr. Mackarey’s Health & Exercise Forum – every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's Articles. check out our exercise forum!
The sunny warm weather is conducive to outdoor sports and activities. Countless adults and more especially students out of school for the summer are participating in tennis, soccer, cross country running, gymnastics, and other sports. These student athletes and others who engage in recreational sports and exercise can be vulnerable to excessive training for all the right and wrong reasons. Parents, family members, coaches, teachers, athletic trainers, friends and health providers must be aware of potential for exercise abuse…as part of the “fitspiration” movement.
It takes only a cursory glance through social media to become aware of the “fitspiration” movement. This catchy term may accompany posts of workout videos, pictures depicting physical activity, or pictures of individuals showing off the muscular bodies they obtained through dedication to rigorous exercise regimens. In a sense, exercise and fitness have become trendy in our society, with more strenuous exercise routines being perceived as more impressive. Cars boast bumper stickers with numbers such as “13.1,” “26.2,” or even “50,” referring to the distances so proudly conquered by runners. When we hear a friend has decided to commit to a rigid training schedule to complete a marathon, we are often in awe of their self-control and motivation, wishing we were that dedicated. But can exercise be a bad thing? The answer is complicated. Exercise is one of the best things we can do for our health. I have heard physicians say that if all the benefits of exercise could be bottled up into a pill; pharmaceutical companies would be fighting for the chance to sell it. However, it can get complicated when one’s reasons for exercising stem from a potentially destructive place, rather than a pursuit of health.
Exercise bulimia is a term used to refer to the excessive use of exercise to burn calories or try to keep a low body weight. It is not a medical diagnosis in and of itself, but the notion of using exercise to make up for excessive calorie consumption or maintain an unhealthily low body weight can occur in both anorexia nervosa and bulimia nervosa. Moreover, when excessive exercise occurs in combination with a significantly low body weight, an intense fear of gaining weight, a disturbed body image, undue influence of body shape on self-worth, or a failure to recognize the seriousness of the condition, an individual would meet the criteria for anorexia nervosa.
Anorexia nervosa can cause serious complications in all body systems. Some examples include disrupted functioning of the heart, reduced lung capacity, hormonal imbalance, amenorrhea, (loss of the menstrual period in women), changes in brain structure, and in severe cases, difficulty with memory. The hormonal changes associated with amenorrhea, especially when coupled with extreme exercise, can lead to reduced bone density and can put women at high risk of stress fractures. Stress fractures are breaks in the bone that occur from overuse through large amounts of exercise rather than the traumatic bone breaks we typically think of where an obvious event results in a broken bone.
Because exercise bulimia can be a part of an eating disorder with potentially life-threatening consequences, it is important to be aware of the warning signs that someone’s exercise routine might be part of an eating disorder. Signs of exercise bulimia may include:
While the definition of exercise bulimia implies a voluntary engagement in excessive exercise for weight loss, my experience from being on female track and cross country teams in high school and college has shown me that anorexia nervosa does not always fit the mental picture we may have of someone who refuses to eat at all or even of exercise bulimia where an individual compulsively engages in excessive exercise. During cross country, the mileage we ran likely would have been considered excessive by the average person. Our team often trained 7 days a week with run-length ranging from 5-12 miles. Most runs were at least 7 miles, and some of my teammates had long runs in excess of 12 miles. The men on our team ran even farther. In hindsight, one of my teammates may have met the criteria for a diagnosis of anorexia nervosa. Her weight was significantly below normal, she feared weight gain, did not eat sufficient calories to replenish what she burned on runs, and despite knowing she was thin, did not fully recognize the potential health consequences due to her low weight. However, it was not a clear cut problem. She was not an obvious candidate for an eating disorder because she was not pursuing the excessive exercise; she was simply following her coach’s training plan. If she did not exercise to the extent she did, the amount of food she ate would have been considered normal, so seeing her eating habits alone did not trigger any red flags. Finally, cross country runners are known for being lean, often even emaciated; it was a common side effect of the sport often not given a second thought. Thankfully, this runner never fell victim to the dangerous downward spiral that is sometimes seen in patients with anorexia nervosa. However, it is important to be aware of the unsuspecting ways in which an eating disorder can sometimes present.
Treatment of eating disorders typically involves a multi-pronged approach with nutritional counseling, psychotherapy, and general medical care playing a role. The nutritional counseling aims to help the patient restore a healthy diet to attain a healthy weight, the psychotherapy aims at getting to the root of the issues that may have contributed to the onset of the eating disorder, and general medical care may be necessary to manage any complications from the eating disorder depending on its seriousness. Educational programs about eating disorders and risk factors have also been shown to be successful in helping to prevent eating disorders.
It can sometimes be a fine line between a healthy passion for exercising and eating well and the start of an eating disorder. Especially in athletes where extreme exercise is part of the sport and putting in extra training is rewarded, it is valuable to be aware of the signs and symptoms of exercise bulimia to help prevent a loved one from crossing over that line. Though serious health consequences are possible in the setting of an eating disorder, treatment and recovery are very possible.
GCSOM Guest Author: Mary Pelkowski, Geisinger Commonwealth School of Medicine MD Class of 2022.
For More Information: www.nationaleatingdisorders.org
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Paul's articles, check out our exercise forum!
What medical problem does a carpenter, typist, truck driver, jackhammer operator, violinist, pianist and court stenographer have in common? Carpal tunnel syndrome! Over the past 10-15 years, carpal tunnel syndrome has moved to the forefront in medicine and has become water cooler conversation. So what is carpal tunnel syndrome and how is it treated?
Carpal tunnel syndrome (CTS) is a nerve disorder caused by compression of the median nerve at the wrist. The median nerve is one of three main nerves that provide sensation to the hand. This nerve specifically supplies sensation to the thumb, index, middle, and half of the ring finger. In CTS, compression on the median nerve occurs as it travels through a narrow passage in the wrist called the carpal tunnel. The carpal tunnel is formed by eight bones in the wrist (the floor of the tunnel) and the transverse carpal ligament, a strong ligament traveling across the roof of the tunnel. Within the tunnel there are nine tendons, which are a bit smaller than a pencil. These tendons share this space with the median nerve. In the case where there is swelling on the structures in the carpal tunnel, a person can experience pins and needles, numbness, and aching in the hand.
To be properly diagnosed, a physician will discuss your symptoms and medical history, and examine strength and sensation. A nerve conduction study, electromyography (EMG), and x-ray may be ordered to provide information regarding sensation in the median nerve distribution and confirm compression at the carpal tunnel.
Treatment focuses on the causes. Therefore treatment suggestions may include activity modification and postural changes during activities. Other suggestions may include frequent rest periods, elevation, and exercises or stretching. Wrist splints are effective in relieving compression at the carpal tunnel and are typically recommended for night wear. Appropriate fit of the splint is vital. Occupational and physical therapists or certified hand therapists can check the fit of pre-fabricated splints or can fabricate a custom splint. The above mentioned treatments all focus on decreasing inflammation and compression on the median nerve.
Your physician may order pain relievers or anti-inflammatory medication. A cortisone injection into the carpal tunnel may also be recommended to assist with decreasing inflammation near the carpal tunnel.
A referral to an occupational or physical therapist or certified hand therapist may be made. A therapist can provide information regarding the diagnosis, appropriate treatment, and symptom reduction. They can make recommendations to introduce into daily activities to allow appropriate positioning of the upper extremities. A therapist will also instruct individuals on helpful stretching exercises or fabricate a wrist splint. Other treatments include ultrasound, iontophoresis, and massage. The focus of therapy is to introduce changes and interventions that reduce inflammation at the carpal tunnel to assist with symptom relief.
Surgery, referred to as a carpal tunnel release, may be indicated if symptoms are significant and impair functional activity performance.
To reduce your chances of getting CTS:
Guest Contributor: Nancy Naughton, OTD, CHT, is a doctor of occupational therapy and certified hand therapist, specializing in the rehabilitation of the hand and upper extremity at Hand Surgery Associates, Olyphant, PA.
NEXT WEEK! Read Dr. Mackarey’s "Health & Exercise Forum" – every Monday
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For of Dr. Paul's article, check out our exercise forum!
A local high school teacher came to my office with weakness and numbness on one side of her face. This well-groomed, attractive middle-aged woman was unable to smile, frown, pout, speak, or eat with facial symmetry. She suffered from a cold, on and off, for about two months. It was not a bad cold, but it would not go away. One day in early summer, while engaged in bird watching, one of her favorite pastimes, she noticed that she could not look through her binoculars. She noticed that her eye would not open and close at will. The next day she woke with ear pain, flaccid muscles on one side of her face, and an inability to close her eye. She had difficulty speaking with clarity due to weak mouth muscles and feared she had a stroke.
She immediately saw her family physician who determined that she had shingles in her ear and developed Bell’s palsy. She was prescribed a steroid anti-inflammatory (Prednisone), antiviral medicine (Acyclovir), and a topical cream (Zovirax). Once she got over the initial fear and shock, she was grateful that her problem of facial weakness was not due to a more serious problem, such as a stroke or brain tumor. She began physical therapy and improved slowly. Her story, along with many other patients, reminded me of the need to raise awareness about cause, diagnosis, symptoms, complications and treatment of Bell’s palsy.
Bell’s palsy, a facial nerve paralysis, occurs when the nerve that is responsible for the movement and sensation of the muscle and skin of the face becomes damaged. The end result of this damage is paralysis of the muscles and numbness of the skin on one side of the face. Typically, the first sign of this disorder is the inability to close one eye or smile on one side of the face. While this problem can occur in any age group, it is rarely seen in people less than 15 or more than 60 years of age. The good news is that most people show signs of improvement within 3-4 weeks and have complete recovery in 4-6 months. The bad news is that reoccurrence can occur on the other side of the face in approximately 10 percent of those affected.
Bell’s palsy is caused by a viral infection. The most common virus is the herpes simplex virus, the same virus that causes cold sores and genital herpes. Other viruses that can cause Bell’s palsy are herpes zoster virus that causes chicken pox and shingles and Epstein-Barr virus, which causes mononucleosis, and cytomegalovirus. When one of these viruses causes inflammation to the facial nerve, it becomes swollen and irritated in the narrow tunnel of bone by the ear. As pressure on the facial nerve increases, damage progresses to the point that the muscles and skin of the face are unable to receive messages from the nerve, leading to paralysis, numbness and other symptoms.
The hallmark symptom of Bell’s palsy is sudden onset of facial muscle weakness and numbness on one side of the face. As a result, it is difficult to close the eye and smile on the weak side. Other symptoms on the affected side can include: the inability to make facial expressions, speak clearly (especially vowel sounds), diminished sense of taste, pain in the area of the jaw or ear, sensitivity of sound, headaches, and changes in production of tears and saliva.
While Bell’s palsy can occur in anyone, it is more common among those who are: pregnant, (especially during the third trimester or first week after birth), diabetic, or suffering from a cold or flu. Also, some research suggests that there may be a genetic predisposition to this problem.
In mild cases of Bell’s palsy, symptoms are completely resolved within 4-6 weeks. As mentioned before, most cases resolve in 4-6 months. However, recovery for those with complete paralysis may vary. For example, permanent facial weakness, facial muscle twitching, and visual problems due to the inability to close the eye, can occur.
Contact you primary care physician immediately, because these symptoms may be associated with a more serious medical condition such as a stroke. Remember, most people with Bell’s palsy make a complete recovery, but early intervention can expedite the process. In severe cases, a neurologist may be consulted. Two commonly used medications are corticosteroids and antiviral drugs. Corticosteroids such as prednisone are strong anti-inflammatory drugs used to reduce the swelling and inflammation on the facial nerve. Antiviral drugs such as acyclovir are used to stop the viral infection that may have caused the inflammation. Studies show that these drugs, when used in combination, are most effective when administered in the first 3 days of the appearance of symptoms.
Physical therapy can also assist in the restoration of facial muscle recovery. Ultrasound with anti-inflammatory drugs, electric stimulation, massage and exercise are commonly performed. While the use of electric stimulation has limited support in the literature, a home exercise program that concentrates on facial muscles, is an essential part of the therapy program. Some simple exercises performed in front of a mirror are: raise eyebrows, bring eyebrows together, open/close eye, fill cheeks with air, suck in cheeks, smile, frown, whistle, say vowels.
Surgery, to relieve pressure on the nerve by removing bone, is rarely performed. Plastic surgery, to improve the appearance of the face, may be an option in cases with permanent paralysis.
Sources: Mayo Clinic; WebMD
NEXT WEEK! Read “Health & Exercise Forum” – Every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is an Associate Professor of Clinical Medicine at GCSOM.
For all Dr. Paul's articles, visit our exercise forum!
“The woods are lovely, dark, and deep,
But I have promises to keep,
And miles to go before I sleep,
And miles to go before I sleep.” Robert Frost
The purpose of this column is to present an alternative to traditional running that will allow training on more interesting and less stressful surfaces such as those used when hiking, mountain biking and horse riding trails in the beautiful woods of Northeast Pennsylvania…”trail running!”
I remember my trail running days with fondness. One day, when the temperatures soared above 90 and my wife pleaded with me to avoid running in the heat (she was wise), as a typical runner, I needed hit the road. As I set out on State Road 348 just on the periphery of Lackawanna State Park in Dalton, the sun was beating down on me. I happened to see a sign that read, “Orchard Trail, Bull Hill Trail, Tree Line Trail.” I thought it might be a good idea to find some shade and decided to run on this path normally used for hiking, mountain biking and horseback riding. It turned out to be a great decision. While I was forced to run 25% slower due to the uneven terrain (rocks, tree roots, stumps), I was able to practice “light running” techniques by running with short strides on the balls of my feet. I felt much more refreshed as I avoided the direct sunlight under the cover of the trees.
Furthermore, I enjoyed the up close view of nature as I ran by cool streams and wet mossy rocks. I saw beautiful flowers, rhododendron, and mountain laurel. I observed deer, chipmunks and birds. In my quest to avoid the hot sun, I discovered the beautiful underworld of “trail running” – a growing trend in today’s running community. If you, like me, enjoyed pounding the pavement for many years, trail running can help you rediscover why you love to run. It is beautiful, peaceful, natural and unique. It is fun to get in touch with your inner child as you run in the woods and get muddy. Trail running makes running fun…and it’s good for your joints!
The trail running community purports that trail running is popular because it satisfies a primal need for man to move through nature, derived from hunter/gatherer days. Others who promote trail running feel the popularity is due to the many advantages it offers. One, trail running prevents impact injuries due to soft surfaces. Two, the training style of running with shorter strides on the ball of the foot, lessens impact. Three, this type of running will develop stronger ankles and trunk core muscles while improving balance, coordination and proprioception from running on uneven surfaces. Lastly, the ability to release copious amounts of endorphins while breathing fresh air instead of roadside fumes is invaluable.
Sources: American Trail Running Association, Trailspace.com
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Paul's articles. check out our exercise forum!
Memorial Day is the unofficial kickoff to summer…outdoor furniture is out, the grill is fired up and the pool is open! This summer try to think of your pleasure puddle in different light…a health spa! It may very well be the exercise of choice for many people. Many have discovered the benefits of moving their limbs in the warm water of a home pool following knee or shoulder surgery. Also, long distance runners who often look for cross training methods without joint compression and arthritis sufferers who are often limited in exercise choices by joint pain from compressive forces when bearing weight, can enjoy the buoyancy effects of water. These are good examples of the benefits or water exercise…aerobic and resistive exercise without joint compression.
Most doctors recommend some form of exercise with arthritis. Pain and fatigue are the most limiting factors for the person with arthritis. Pool exercise may be the answer. With proper technique, adequate rest periods, appropriate resistance and repetitions, water exercise can be very effective.
The following are some of the benefits of water exercise:
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our Health and Exercise Forum!
Since 1949 May has been designated as National Mental Health Month for the purpose of eliminating the stigma associated with mental illness by raising awareness. One of the most common mental health conditions is depression. New research from Boston University School of Public Health has found that depression has been increasing in the United States and life with COVID for more than two years has accelerated it rapidly. In 2021 the number of people suffering from depression increased more than 32 percent, affecting 1 in every 3 American adults. However, research also has good news to offer: one of the most understated benefits of exercise is mental health! Specifically, aerobic exercise (exercise that increases your heart rate for 30 minutes or more) such as walking, biking, running, swimming, hiking, elliptical & stepper machines to name a few, is the secret to “runner’s high.” This exercise euphoria is not limited to runners alone, but all who engage in aerobic exercise are more likely to experience high energy, positive attitude, and mental wellness.
Physical activity, specifically aerobic exercise, is a scientifically proven useful tool for preventing and easing depression symptoms. Studies in the British Journal of Medicine and the Journal of Exercise and Sports Science found that depression scores were significantly reduced in groups that engaged in aerobic running, jogging or walking programs, 30-45 minutes 3-5 days per week for 10-12 weeks when compared to a control group and a psychotherapy counseling group.
Depression is the most common mental disorder and is twice as common among women as in men. Symptoms include: fatigue, sleeplessness, decreased appetite, decreased sexual interest, weight change, and constipation. Many of these symptoms are likely to bring an individual to their family physician.
According to research, exercise reduces depression in two ways, psychologically (mentally) and physiological (physically).
Psychological or Mental Benefits of Exercise on Depression:
Physiological or Physical Benefits of Exercise on Depression:
NEXT MONDAY - Read Dr. Paul J. Mackarey’s "Health & Exercise Forum"!
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's Articles, check out our Health and Exercise Forum!
Summer (and Memorial Day, the kickoff of the gardening season) will be here soon and gardeners in northeast PA are anxious work in their gardens and enjoy the fruits of their labor. Last week, Health & Exercise Forum presented tips for gardeners for preventing hand and arm injuries such as carpal tunnel syndrome. This week’s column is dedicated to prevention of lower back and lower body injuries when working in the yard and for gardeners with disabilities.
A relaxing and enjoyable activity for many, gardening can turn dangerous without proper precaution as repetitive stress injuries, back pain, muscle pulls, can stem from raking, weeding, digging and pruning, can turn into serious problems if not treated appropriately. Since prevention is the best approach, the US Dept of Agriculture promotes warm-up exercises and injury prevention tips to help all levels of gardeners avoid serious and long-term injuries while enjoying this popular outdoor activity.
People with various disabilities enjoy gardening at different levels. For example, those suffering from neurological diseases with muscle weakness, paralysis and poor balance as well as those with musculoskeletal problems such as neck and LBP or hip and knee arthritis can safely enjoy gardening at some level. This outdoor labor of love is very therapeutic.
Warm up and stretching is important. Don’t garden first thing in the morning before you have a chance to warm up. Get up, go for a short walk, have breakfast and maybe warm up with a hot shower before working in the garden. Some stretches include:

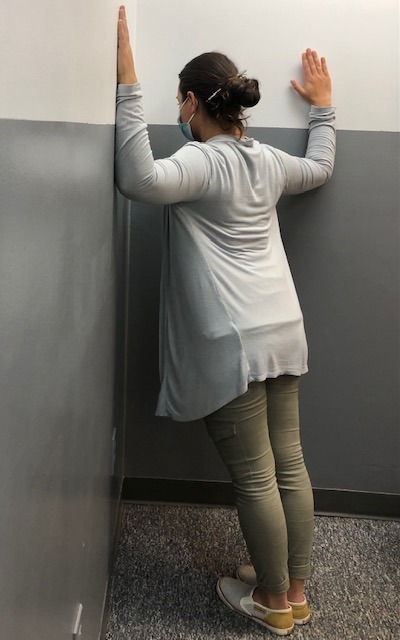
Corner Stretch: Stand facing a corner wall with arms and shoulders at 90 degrees. Lean into corner and stretch shoulders and back. (PHOTO 1)
Knees to Chest Back Stretch: While lying on your back, bring both knees up towards your chest. (PHOTO 2)
Note: These exercises should never be painful when completing them. You should only feel a gentle stretch. Hold the stretch10 seconds and repeat 5 times before you garden and every 2-3 hours while working. Should you experience pain, please consult your family physician or physical therapist.
Source: Karen Funkenbusch, MA; Willard Downs, PhD.: U. S. Department of Agriculture - Agricultural Engineering Extension
Model: Ashley Ottaviani, PTA
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. Access all of Dr. Mackarey's articles at our Health and Exercise Forum!
