Studies have shown a recent escalation of joint replacements in a much younger and more active group than previously noted…the baby boomer! While the end result is mostly physical, the cause is often psychological. We all know the personality type: type A, hyperactive, goal-oriented, driven, possessed and highly organized – almost at all costs! Many of you have seen fitness enthusiasts running through the streets at 5:30 AM for 5-10-15 miles each day. Moreover, many of these runners have more activities planned later in the day: golf, tennis, ski, swim, play sports with their kids. Well, after 20 years of this behavior, many of these enthusiasts are now suffering the effects of long term multiple micro traumas. They are suffering from what orthopedic surgeons at the University of Pennsylvania call “Boomeritis! Boomeritis is inflammation of the baby boomer from overuse. Lower back pain, hip, groin, and knee pain is almost a daily event.
As baby boomers continue to enjoy sports with the same vigor and intensity as when they were younger, they are finding that their older bodies just can’t keep up. While these individuals often succeed in finding the balance of fitness and craziness, they have had times when they took it too far. Furthermore, nearly all compulsive exercisers suffer from over training syndrome. When take too far compulsive behavior is rationalized by insisting that if they didn’t work to extreme then their performance would suffer.
*Each sign is worth 1 point:
If you have two or more of the warning sings, consult your family physician to rule out potentially serious problems.
Avoid weight bearing exercises two days in a row. Run one day, walk, swim or bike the next.
Use the elliptical instead of the treadmill.
Avoid squatting…deep squatting is bad for your hips and knees. Even when gardening, use a kneeling pad instead of bending down and squatting.
Visit your family doctor regularly and listen to your body.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's articles, visit our exercise forum!
Fall is here, cross-country running season has begun and the 26th Steamtown Marathon is only a few weeks away! With that in mind, running injuries, some very specific to women, are on the increase…
While driving to or from work have you noticed more local running enthusiasts in the past few years? Moreover, have your noticed that most of the runners are women? Scranton Running Company has contributed to NEPA’s participation in a national trend; more women are engaged in running than men! Female runners account for 9.7 million runners (57%) while 7 million males run on a national level.
With this surge, the female runner has been subjected to a host of related injuries, including shin splints, which often lead to stress fractures. New research has found that stress fractures may be related to the loss of weight and body mass associated with the sport.
A recent study from Ohio State University found that female runners with a Body Mass Index (BMI) below 19 may have a higher risk of developing stress fractures than women with a BMI of 19 or above. Furthermore, the study also found that these women took longer to recover from these injuries.
According to Timothy Miller, MD, “When body mass index is very low and muscle mass is depleted, there is nowhere for the shock of running to be absorbed other than directly into the bones. Until some muscle mass is developed and BMI is optimized, runners remain at increased risk of developing a stress fracture,”
The study also found that female runners with a BMI of 19 or higher with severe stress fractures required 13 weeks to recover from their injuries and return to running. Runners with a BMI lower than 19, however, took more than 17 weeks to recover.
They concluded that women should know their BMI and consult with a medical professional to maintain a healthy number. Additionally, women should cross-train and include resistance training to improve the strength and muscle mass of the lower extremities to prevent injury.
The current BMI wisdom, according to the National Institutes of Health, is 19.8 for men and 24 for women, however, strong and competitive women tend to have a BMI of 26. A BMI of 18 is considered malnourished.
Body mass index (BMI) is a measure of body fat based on height and weight of adult men and women over 20 years of age, according to the National Institutes of Health.
BMI = (weight in pounds / height in inches squared) X 703)
Example 1: a person who weighs150 pounds and is 68 inches (5 feet 8 inches) tall has a BMI of 22.8
Example 2: a person who weighs 110 pounds and is 66 inches (5 feet 5 inches) tall has a BMI of 17.7
Underweight < 18.5%
Normal weight 18.5 to 24.9%
Overweight 25 to 29.9%
Obesity 30 and over
A stress fracture is fatigue damage to bone with partial or complete disruption of the cortex of the bone from repetitive loading. While standard x-rays may not reveal the problem, a bone scan, and MRI will. It usually occurs in the long bones of the leg, mostly the tibia (shin bone) but also the femur (thigh) and foot. Occasionally, it occurs in the arm.
FEMALE RUNNERS WITH BMI LOWER THAN 19 – is a primary risk factor.
10-21% of all competitive athletes are at risk for stress fractures. Track, cross country and military recruits are at greatest risk. Females are twice as likely as males to have a stress fracture. Other athletes at risk are: sprinters, soccer and basketball players, jumpers, ballet dancers are at risk in the leg and foot. Gymnasts are also vulnerable in the spine while rowers, baseball pitchers, golfers and tennis players can experience the fracture with much less frequency in the ribs & arm.
The problem is much more prevalent in weight bearing repetitive, loading sports in which leanness is emphasized (ballet, cheerleading) or provides an advantage (distance running, gymnastics).
Stress fractures usually begin with a manageable, poorly localized pain with or immediately after activity such as a shin splint. Over time, pain becomes more localized and tender during activity and then progresses to pain with daily activity and at rest.
Source: Ohio State University, Science Daily
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy!
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Paul's Articles, visit our exercise forum!
Ankle swelling is a common symptom that occurs when your body retains fluid in the lower legs, ankles and feet. Most people have experienced it at some point in their lives and it often resolves on its own with elevation and muscle movement. While it is usually benign and occurs on both sides of the body, in some instances immediate medical attention is required. The most common causes of ankle swelling are:
Prolonged Positions – you have probably noticed swelling in your ankles and feet after a long trip by plane or car. Some may also experience symptoms after a long day at work sitting or standing in one position for an extended period of time. It may be the most common cause of lower leg swelling and easiest to resolve.
Diet- excessive salt in your diet is associated with swelling in the lower legs, especially when associated with other risk factors for swelling such as organ function or obesity.
Varicose Veins – when the valves in the blood vessels which carry blood from the legs back to the heart are damaged, blood and fluid can collect in the lower legs. Prolonged standing or sitting without intermittent movement with worsen the condition.
Pregnancy – during pregnancy, the body retains more fluids than usual and most women experience some form of swelling in the lower legs, ankles and feet.
Medications – certain drugs can cause fluid retention in the lower legs such as: anti-inflammatory medications, steroids, diabetes medications, antidepressants and cardiac medications.
Blood Clots – blockages in the blood vessels of the lower leg can limit the movement of fluid from the legs back to the heart. It is often present in only one leg and associated with warmth, pain, and cramping. It is a serious condition and requires immediate medical attention.
Trauma/Infection – after a trauma or injury such as an ankle sprain, bruise or fracture, the damaged tissue leaks fluid surrounding the affected area. Also, when specific area of the lower leg can becomes infected, as in the case of a cut or splinter in the ankle or foot that has not healed properly, swelling occurs in the surrounding tissues. These situations are often associated with warmth, pain and limited to the side of the injury. Treatment to injured tissues and the infection is required.
Lymphedema – swelling in the lower leg can occur when there is a blockage in the lymphatic system is blocked or when lymph nodes are removed in surgery for cancer. Medications, massage, compression garments, and elevation, can address the symptoms.
Obesity – due to the excessive weight placed on the tissues of the legs, ankle and feet and adipose tissue in the abdomen compressing blood vessels, obesity is one of the most common causes of lower leg swelling. It also complicates all of the above conditions associated with swelling in the legs.
Diseases – such as those of the kidney, heart, and liver are associated with swelling in the lower legs.
Change Positions – on a long plane ride or sitting all day at school or work – get up and walk around every 30-45 minutes. Set a timer on your phone to remind you.
Exercise – regular exercises keeps the muscles and blood vessels in you lower extremities healthier. Also, intermittent movement of the leg muscles throughout the day, even when sitting, serve to prevent swelling. Try ankle pumps and toe curls.
Elevation – when sitting or lying down, try elevating your ankles and feet on a pillow to allow gravity to assist fluid movement in your legs.
Low-Sodium Diet – read the labels on your food and you will be shocked by how much sodium is in most foods, especially canned soups and vegetables. But, there are low-sodium options and don’t add more salt to your food.
Weight Loss – maintaining a healthy BMI is the single best thing you can do, not only for lower leg swelling, but for your overall health and wellness.
Compression Socks – for most people, over-the-counter compression socks will adequately prevent fluid retention in the lower legs. For comfort, begin with the lightest compression possible. 12-15 or 15-20 mm of mercury is a good start and put them on as soon as you get up in the morning, before swelling begins.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in ”The Sunday Times - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Paul's articles, check out our exercise forum!
Fall in NEPA is one of my favorite times of year. For outdoor enthusiasts, there is nothing more refreshing than activities in the bright sunshine and crisp, clean air. The hot humid summer weather can be a deterrent to outdoor activities and this time of year provides an opportunity to get fit by beginning a walking program. For many who have not maintained an active lifestyle or have health issues, it is challenging to know where to begin. Moreover, beginning without a good plan can lead to injury and leave you discouraged. For example, those overweight and de-conditioned should not start a walking program too aggressively. Walking at a fast pace and long distance without gradually weaning into it will most likely lead to problems.
There is probably nothing more natural to human beings than walking. Ever since Australopithecus, an early hominin (human ancestor) who evolved in Southern and Eastern Africa between 4 and 2 million years ago, that our ancestors took their first steps as committed bipeds. With free hands, humans advanced in hunting, gathering, making tools etc. while modern man uses walking as, not only a form of locomotion, but also as a form of exercise and fitness. It is natural, easy and free...no equipment or fitness club membership required!
“There’s no question that increasing exercise, even moderately, reduces the risks of many diseases, including coronary heart disease, breast and colon cancer, and Type 2 diabetes,” said Dr. Jennifer Joyce, MD, professor of family medicine at GCSOM. “Research has even shown that you could gain two hours of life for each hour that you exercise regularly.” According to the American Heart Association, walking as little as 30 minutes a day can provide the following benefits:
Anything is better than nothing! However, for most healthy adults, the Department of Health and Human Services recommends at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity, or an equivalent combination of moderate and vigorous aerobic activity. The guidelines suggest that you spread out this exercise during the course of a week. Also aim to do strength training exercises of all major muscle groups at least two times a week.
As a general goal, aim for at least 30 minutes of physical activity a day. If you can't set aside that much time, try several short sessions of activity throughout the day (3 ten or 2 fifteen minute sessions). Even small amounts of physical activity are helpful, and accumulated activity throughout the day adds up to provide health benefit.
Remember it's OK to start slowly — especially if you haven't been exercising regularly. You might start with five minutes a day the first week, and then increase your time by five minutes each week until you reach at least 30 minutes.
For even more health benefits, aim for at least 60 minutes of physical activity most days of the week. Once you are ready for a challenge, add hills, increase speed and distance.
Keeping a record of how many steps you take, the distance you walk and how long it takes can help you see where you started from and serve as a source of inspiration. Record these numbers in a walking journal or log them in a spreadsheet or a physical activity app. Another option is to use an electronic device such as a smart watch, pedometer or fitness tracker to calculate steps and distance.
Make walking part of your daily routine. Pick a time that works best for you. Some prefer early morning, others lunchtime or after work. Enter it in your smart phone with a reminder and get to it!
Studies show that compliance with an exercise program is significantly improved when an exercise buddy is part of the equation. It is hard to let someone down or break plans when you commit to someone. Keep in mind that your exercise buddy can also include your dog!
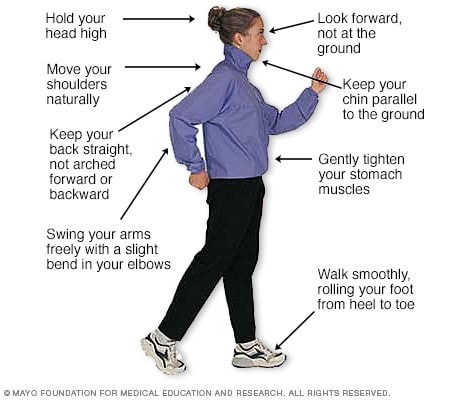
Like everything, there is a right way of doing something, even walking. For efficiency and safety, walking with proper stride is important. A fitness stride requires good posture and purposeful movements. Ideally, here's how you'll look when you're walking:
Visit your doctor regularly and listen to your body.
Sources : Sapiens.org; WebMD; Mayo Clinic
NEXT MONDAY BLOG and in print in THE SUNDAY TIMES TRIBUNE – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Paul Mackarey's articles, check out our exercise forum!
There is little doubt that the workplace has been redefined since the pandemic as many employees continue to work from home. Sitting for many hours at a workstation that may not be optimal has also changed the way we define workplace health and safety. It may be more important than ever to pay close attention to designing an ergonomic workstation, changing position, and stretching regularly to prevent injury.
Since 1894 Labor Day has been designated as the national holiday that pays tribute to the contributions and achievements of American workers. Research supports the notion that healthier employees are happier and more productive. When employers encourage healthy behavior and safety at work, they benefit in many ways. For example, in addition to improving job satisfaction and productivity, healthy employees save money by using less sick time, worker’s compensation benefits and health benefits. For example, according to the Centers for Disease Control and Prevention, approximately 75 percent of employers” health care costs are related to chronic medical problems such as obesity, diabetes, high blood pressure, and high cholesterol. De-conditioned, overweight employees are more likely to suffer from these preventable conditions and are at greater risk for injury. Employers, please consider using this holiday as an opportunity to start a health promotion program at your workplace…have a health fair, offer healthy snacks, encourage walking, smoking cessation, exercising at lunch, and offer fitness club stipends.
Lower back pain, one of the costliest illnesses to employers, is one example of a problem which can be prevented with a good health and safety program. It is widely accepted in the medical community that the best treatment for lower back pain (LBP) is prevention. Keeping fit, (flexible and strong), practicing good posture, and using proper body mechanics are essential in the prevention of LBP. At our clinic, significant time and effort is spent emphasizing the importance of these concepts to our patients, employees, and the businesses we work with through industrial medicine programs. A comprehensive approach can produce significant reductions in LBP injuries through an onsite safety program which promotes education, wellness, body mechanics, lifting techniques, postural and stretching exercises and ergonomics.
As little as 10 extra pounds puts great stress on your lower back. It also makes it more difficult to maintain good posture. Eat well, exercise regularly and don’t smoke. Smokers have a much higher incidence of LBP and failure from lower back surgery.
Good posture is critical for a healthy back. When sitting, standing or walking maintain a slight arch in your lower back, keep shoulders back, and head over your shoulders. In sitting, use a towel roll or small pillow in the small of the back. Also, consider sitting on a physio ball, which promotes proper posture for part of the day.


Perform postural exercises throughout the day. Most of the day we sit, stand, and reaching forward and bend our spine. These exercises are designed to stretch your back in the opposite direction of flexion. Please perform slowly, hold for 3-5 seconds and repeat 6 times each 6 times per day.
Chin Tuck: Tuck your chin back to bring your head over shoulders.
Shoulder Blade Pinch: Pinch your shoulder blades together.
Standing Extension: While standing, put your hands behind back and extend lower back 10-20 degrees.
Good Body Mechanics and ergonomics are also important in the prevention of LBP. When lifting, think twice. Think about the weight, shape and size of the object. Think about where the object is going and the surface resistance of the floor. Does it require two people to lift? Can I safely lift that high or bend that low?
When bending to lift an object think about safety:
Proper Lifting Technique:
Visit your doctor regularly and listen to your body.
Model: Lexi DiGregorio, PTA
NEXT SUNDAY IN THE PAPER AND EVERY MONDAY'S BLOG – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Paul's articles, check out our exercise forum!
“Everybody talks about the weather, but nobody does anything about it,” said Mark Twain. Just ask 93% of the arthritis sufferers who believe that the weather affects their pain level. History tells us that Benjamin Franklin, Leonardo da Vinci, and Christopher Columbus also felt this way about the weather.
Patients at our clinic have been particularly sensitive to joint pain on cold, damp days, especially during the past few weeks. In my clinical practice of orthopedic and sports physical therapy, an informal survey found that 95 out of 100 patients (95%) with arthritis reported increased pain with weather changes. While most people report that the coldness and dampness seem to irritate their joints, they also report more pain with weather changes in the summer. There is a reasonable explanation…
Joints in the body have a lining called synovium that secretes a lubricating fluid called synovial fluid. In joints with arthritis, there is an overproduction of synovial fluid. In theory, when the barometric pressure changes, so to will the pressure inside your joints, especially if it is already overfull with extra fluid from arthritis. This added pressure stimulates the nerve endings in the joint to produce inflammation and pain.
Despite this overwhelming response from patients, scientific studies vary in their support of this claim. According to the Mayo Clinic, in 1961, a famous arthritis doctor (rheumatologist), built a climate chamber and discovered that when high humidity was combined with low barometric pressure, patients reported increased joint pain and stiffness. A recent study found that changes in barometric pressure and cooler temperatures are associated with joint pain. However, other studies have found increased joint pain with high barometric pressure in both warm and cold weather while another study found pain with low pressure.
What does this mean? It means that patients with arthritis consistently report pain with weather changes but science has not found an accurate method to consistently support these claims. Some of these inconsistencies may be attributed to the fact that there are differences in sensitivity among individuals. For example, some patients have symptoms before the weather changes, while others notice symptoms during or after the weather changes. Still yet, some report more pain in colder conditions while others notice more pain in warmer weather. It appears that changes in the weather, such as a high to a low or warm dry to cold damp and vice versa is the culprit when it comes to irritating arthritis in a joint.
If I have arthritis, should you move to Arizona? Yes and no! Yes, the warm and dry climate of Arizona will probably make you feel better overall. However, it will not cure the degenerative changes in your joints and you may still have pain when CHANGES in the weather occur. This is proven to be true by the fact that there are many very busy rheumatologists in Arizona!
In conclusion, it is safe to say that there is some evidence to support the claim that most patients with arthritis have increased symptoms of joint pain and stiffness with CHANGES in the weather:
Therefore, each patient must be individually evaluated by their physician to determine the extent of their arthritis and its relationship to the changes in the weather. While the cause of their increased symptoms with changes in the weather may not be completely understood, each patient must determine the adjustments in their lifestyle and/or medications according to the particular weather patterns that affect their problem most.
Visit your doctor regularly and listen to your body.
NEXT SUNDAY IN THE PAPER AND EVERY MONDAY'S BLOG – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is repeated every year at this time with the intent of raising the level of awareness to prevent death or serious illness from heat stroke in athletes and other active people in hot, humid weather.
It is August and summer is rapidly passing! So, get outdoors and have fun in the sun. However, please be mindful of how your body reacts to high humidity and heat and take appropriate precautions. Athletes are particularly vulnerable this time of year due to daytime practice sessions. (August 7, 2023, first day of acclimatization and August 14, 2023, first day of practice for fall sports according to PIAA). Visit www.piaa.org for more information. Keep in mind, you don’t have to be running a marathon or playing football in full uniform to suffer from heat stroke.
Heat stroke, one of the most serious heat-related illnesses, is the result of long term exposure to the sun to the point which a person cannot sweat enough to lower the body temperature. The elderly and infants are most susceptible and it can be fatal if not managed properly and immediately. Believe it or not, the exact cause of heat stroke is unclear. Prevention is the best treatment because it can strike suddenly and without warning. It can also occur in non athletes at outdoor concerts, outdoor carnivals, or backyard activities.
Some “old school” folks think that wearing extra clothing and “breaking a good sweat” is an optimal goal for exercise. However, it may be potentially very dangerous in hot and humid conditions. When exercising in hot weather, the body is under additional stress. As the activity and the hot air increases your core temperature your body will to deliver more blood to your skin to cool it down. In doing so, your heart rate is increased and less blood is available for your muscles, which leads to cramping and other more serious problems. In humid conditions, problems are magnified as sweat cannot be evaporated from the skin to assist in cooling the body.
The American Academy of Pediatrics and The American College of Sports Medicine has the following recommendations which are appropriate for both the competitive athlete and weekend warrior:
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, check out our exercise forum!
Can you believe that the 4th of July holiday was more than one month ago? Do not despair! There is still plenty of time to be outdoors in NEPA and experience so many activities such as: biking, hiking, running, walking, swimming, boating, golfing, and playing tennis to name a few. Late summer and early fall tend to be beautiful and is also a wonderful opportunity to discover your inner child, mix it up and try something new! Below are some new and exciting ways to stay active and have fun in the sun:

Spending time on any of the beautiful lakes in NEPA is time well spent. From an exercise standpoint, rowing, canoeing and kayaking offer a very special experience. Most kayaks are light weight, easy to use and maneuverable on a lake. Sitting low on the water offers a unique perspective as you feel yourself gliding across the lake. The Countryside Conservancy, in partnership with Lackawanna State Park, sponsors moonlight kayak events on the lake at the park. With a bright full moon, you can begin at 8 pm and return at 10 pm. Bring bug spray and headlights to enjoy the sunset and moon rise on the lake. You will feel like a kid breaking the rules of the park by being on the water after dark!
NOTE: Try kayaking in the daytime first and then advance to sunset trips before staying on the water for the moonlight. Rentals are available at the park.
Website: www.countrysideconservancy.org; www.dcnr.state.pa.us/stateparks.org

Stand up paddle boarding (SUP) is becoming a fast-growing sport among water enthusiasts. It is a fun way to exercise your core, improve balance, and tone your upper body. It requires minimal equipment; a board that is essentially a long and wide surfboard and a long paddle to use while standing on the board. It can be done in the ocean surf, bay, lakes, or rivers; however, beginners would be wise to stay in calm water. Rentals are available at most beaches.
Check out the video for more information: REI paddleboard basics
What is it? Imagine a standup paddle board with a handlebar and pedals like a exercise stepper machine. Instead of using a paddle, you step up and down on the pedals and fins under the board propel you through the water. Check it out…Hobie Mirage Eclipse Stand Up Peddle Board; Dick’s Sporting Goods
Zumba is a very popular form of dance aerobics spiced up with Latin music. When adding water and sun to this already cool activity, you are assured to have fun while exercising. As with any aquatic exercise, the added resistance from the water gives arm rows and leg kicks more challenge. Female participants report an additional benefit; they are uninhibited to “shake that thing” to the music under the cover of the water. So, beat the heat, let loose and get some fun in the sun while you exercise.
NOTE: Consider trying regular Zumba first to get the hang of it. Amy Sekol is a local certified Zumba instructor and also offers Aqua Zumba. (amys.zumba.com)
Website: www.zumba.com
I love this idea…why didn’t I think of it first! In the gym I enjoy the elliptical machine because it simulates running without the impact on my joints but of course, I would rather be outdoors. Well, this is the answer to my prayers…an elliptical machine that is attached to a bike with handle bars and brakes included. I think it will probably be difficult on steep hills but it is something I MUST TRY!
Website: www.elliptigo.com; www.mywingflyer.com
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
For all of Dr. Mackarey's Articles, check out our exercise forum!
According to the National Institutes of Health, an estimated 19.1% of U.S. adults 18 and older had an anxiety disorder in the past year. Anxiety disorders were higher for females (23.4%) than for males (14.3%). An estimated 31.1% of U.S. adults experience an anxiety disorder at some time in their lives.
There are a wide variety of anxiety disorders and will vary by the objects or situations that induce them. However, the features of excessive anxiety and related behavioral disturbances are similar. Anxiety disorders can interfere with daily activities such as job performance, school work, and relationships. Symptoms include: distress, nausea, shortness of breath, bowel pattern changes, excessive perspiration, frequent laughing or crying, restlessness, and is often associated with depression. While there are many types and degrees of anxiety and there is no substitute for medical and psychological care, there are some simple and basic tools to help manage the problem…daily exercise is one easy, affordable and accessible suggestion for most. Multiple studies have discussed the incidence of unhealthy self management of anxiety, including the use of alcohol and recreational drugs.
Last week, I presented coping tips for the management of anxiety. In this column, I will discuss one of the most understated benefits of exercise – mental health! Specifically, aerobic exercise (exercise that increases your heart rate for 30 minutes or more) such as walking, biking, running, swimming, hiking, elliptical & stepper machines to name a few, is the secret to “runner’s high.” This exercise euphoria is not limited to runners alone, but all who engage in aerobic exercise are more likely to experience high energy, positive attitude and mental wellness.
Physical activity, specifically aerobic exercise, is a scientifically proven useful tool for preventing and easing anxiety and depression symptoms. Studies in the British Journal of Medicine and the Journal of Exercise and Sports Science found that anxiety and depression scores were significantly reduced in groups that engaged in aerobic running, jogging or walking programs, 30-45 minutes 3-5 days per week for 10-12 weeks, when compared to a control group and a psychotherapy counseling group.
According to research reported in sports medicine journals, exercise reduces anxiety and depression in two ways, psychologically (mentally) and physiological (physically).
Psychological or Mental Benefits of Exercise on Anxiety and Depression:
Physiological or Physical Benefits of Exercise on Anxiety and Depression:
Work hard to recognize and overcome these symptoms to begin an exercise program. An aerobic exercise routine should eventually lessen these symptoms.
Visit your doctor regularly and listen to your body.
SOURCES: University of Pittsburgh Medical Center (UPMC); National Institutes of Health (NIH); The American Journal of Sports Medicine
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Paul's articles, check out our exercise forum!
According to the National Institutes of Health, an estimated 19.1% of U.S. adults 18 and older had an anxiety disorder in the past year. Anxiety disorders were higher for females (23.4%) than for males (14.3%). An estimated 31.1% of U.S. adults experience an anxiety disorder at some time in their lives.
There are a wide variety of anxiety disorders and will vary by the objects or situations that induce them. However, the features of excessive anxiety and related behavioral disturbances are similar. Anxiety disorders can interfere with daily activities such as job performance, school work, and relationships. Symptoms include: distress, nausea, shortness of breath, bowel pattern changes, excessive perspiration, frequent laughing or crying, restlessness, and is often associated with depression. While there are many types and degrees of anxiety and there is no substitute for medical and psychological care, there are some simple and basic tools to help manage the problem…daily exercise is one easy, affordable and accessible suggestion for most.
Multiple studies have discussed the incidence of unhealthy self management of anxiety, including the use of alcohol and recreational drugs. The University of Pittsburgh Medical Center (UPMC) recommends the following healthy tips for coping with anxiety:
1. Get Enough Sleep
Adequate sleep is critical for mental health. Unfortunately, anxiety can lead to sleeping problems and, according to the Anxiety and Depression Association of America (ADAA) inadequate sleep can worsen anxiety.
Seven to nine hours of sleep each night is recommended for most adults. The National Sleep Foundation recommends maintaining a regular schedule that includes going to bed at the same time each night and waking up at the same time each morning.
2. Practice Mindfulness Meditation
Incorporating meditation into your life can help you cope with anxiety, according to the National Center for Complementary and Integrative Health.
Research shows mindfulness meditation programs are effective in reducing anxiety and depression. UPMC offers a Mindfulness-Based Stress Reduction Course and a Beginners Guide to Meditation that have been proven to be very effective. Another option for reduction of anxiety and stress is Progressive Muscle Relaxation. This mind-body technique can be found in 5, 10, 15 or 20 minute videos.
3. Spend Time in Nature
How you deal with anxiety should include a walk in the forest or even a tree-lined park. In NEPA we are very fortunate to have access to beautiful walking and biking trails and state parks. Make time to enjoy them.
Research shows that “forest bathing,” long, slow walks in nature for health purposes, can lower blood pressure and relieve anxiety. A review of clinical trials published in the International Journal of Biometeorology found that salivary cortisol levels, biomarkers for stress, were significantly lower in groups who participated in forest bathing versus the control group.
4. Take up Yoga or Tai Chi
Yoga does more than increase your flexibility. It incorporates exercise, deep breathing, and meditation. Yoga is an all-in-one anti-anxiety activity, as shown in a review of body-centered interventions published in Frontiers in Psychology. Tai chi, a mix of meditation and martial arts, works much the same way.
5. Dance Therapy
That same research found that dance therapy, also known as movement therapy, reduces anxiety by engaging the body’s nervous system, which regulates how the body reacts to stress. In addition, dance/movement therapy increases production of serotonin, a chemical produced by the cells that’s responsible for mood.
6. Breathe Through It
When you begin to feel anxiety or a panic attack with symptoms such as: sweating, trembling, dizziness, rapid heartbeat and nausea, start to come on, “take a deep breath.” Research shows that slow deep breaths can calm you down and lower your heart rate while quick, shallow breaths can induce or worsen anxiety.
One breathing technique shown to reduce anxiety is diaphragmatic breathing. Using your diaphragm for deep breathing requires you to fill your lungs to capacity.
Breathe in slowly through your nose so that your stomach rises. Then, tighten the stomach muscles and exhale slowly through pursed lips. Repeat several times.
7. Limit Caffeine and Alcohol
Too much caffeine restricts blood vessels, which can increase blood pressure and contribute to anxiety. Coping with anxiety also doesn’t mean masking it with alcohol. Studies show that there is a complex relationship between alcohol and anxiety. While some may use alcohol and recreational drugs to mask the symptoms of anxiety (often leading to substance abuse disorder), some studies show that alcohol can interfere with the neurotransmitters that manage anxiety and prevent you from getting a good night’s sleep. Drinking to cope creates a sort of feedback loop, which makes the anxiety worse and can lead to alcohol dependence.
8. Check Your Medicine
Certain medicines, such as corticosteroids, asthma drugs, and others, can cause anxiety. Ask your doctor if any medicines you take may be a contributing factor.
9. Eat Healthy Foods
Keeping the body nourished is essential for all functions of life. New research shows that a healthy diet may affect more than just weight and energy levels. One example is a Mediterranean Diet, with lots of vegetables, fruits, beans, lentils, nuts, whole grains, extra virgin olive oil and a moderate amount of fish (especially those rich in omega-3 fatty acids), with limited use of red meat.
10. Keep a Journal
Keeping a journal can be a great way to keep track of your progress with anxiety and how your body responds to such situations. Tracing the triggers of anxiety can help you develop the skills to properly respond when put in anxious conditions.
11. Exercise Regularly
Exercise promotes the release of endorphins. These brain chemicals reduce the body’s reaction to pain and stress. They also produce a feeling of euphoria, or happiness, that’s comparable to morphine. Just five minutes of aerobic exercise can kick start these anti-anxiety effects, according to some studies. Next week in “Health & Exercise Forum” specific details about exercise for anxiety will be presented.
Talk to a Mental Health Professional
Chronic anxiety also can point to an underlying mental health issue. When your anxiety causes extreme distress or interrupts your ability to function on a daily basis, or when panic attacks are frequent and debilitating, it’s important to talk to your physician and ask for a referral to a mental health professional. They can provide a treatment plan, which may include specialized anti-anxiety medicine, psychotherapy, or both.
Visit your doctor regularly and listen to your body.
SOURCES: University of Pittsburgh Medical Center (UPMC); National Institutes of Health (NIH);
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next week: Coping with Anxiety Part II This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM. For all of Dr. Paul's articles, check out our exercise forum!
