One of the greatest frustrations in modern medicine occurs when a safe, tried, and proven treatment exists to prevent deadly disease, but it is not possible to administer it to the potentially vulnerable victims. Over time, the disease unnecessarily spreads exponentially. Malaria in sub-Saharan Africa where one million die from the disease each year and tuberculosis in Haiti where the highest rate in the Western Hemisphere exists, are two examples. Another such disease that can be prevented with vaccination is the Human Papillomavirus, (HPV). While some strains of HPV lead to cancer an almost 100 percent disease prevention rate is associated with those vaccinated before the age of first potential exposure.
Despite validated scientific evidence of safety for more than 15 years, HPV vaccination skepticism not only persists, but is on the increase. Surveys show that the “anti-vaccine” culture fueled by COVID 19 has carried over to other vaccinations, including HPV. For example, provider orders for HPV vaccines decreased 24% in 2020, 9% in 2021 and 12% in 2022 when compared to 2019.
Many parents belonging to the “anti-vaccine movement” justify their actions with completely unfounded and unsupported fears of autism and other illnesses from the vaccine. However, their decisions affect the health of not only their children, but others as well.
According to Paul Offit, MD, professor of pediatrics, division of infectious diseases director of the Vaccine Education Center at the Children’s Hospital of Philadelphia (CHOP), every year in the United States, thousands of men and women die of cancers that can be prevented with a simple vaccine administered during adolescence to prevent HPV. He states, “It is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
The Centers for Disease Control (CDC) has listed the prevention of HPV as a one of its “Top 5 Health Initiatives.” The pressure will be on health care providers to take the time to educate and dispel myths in order for parents to make informed decisions for the health of their children. In fact, local pediatrician Anders Nelson, who spends significant time educating parents and children about the importance of vaccination, requires parents to sign a “Refused HPV Vaccine” form and boasts a 99% compliance rate.
2013 the CDC reported 13.9% of males and 37.6% of females’ ages 13-19 are completing vaccination for Human Papillomavirus (HPV). Despite such low vaccination rates, a 50% reduction in HPV among 14 -19-year-old females was noted. Moreover, studies demonstrate a near 100% success rate to eradicate HPV in children vaccinated between the ages of 9 and 11 years old, leading health professionals to ask a frustrating and burning question: “Why do parents hesitate to vaccinate their children from a potentially deadly virus when a safe and effective cure exists?”
Reasons cited by parents for not vaccinating are challenging to health providers. Some of the most common responses include misunderstanding of HPV and its impact, unfamiliarity with vaccine recommendations, distrust of vaccine safety, religious and moral issues with mode of disease transmission, and social pressures. It will be the purpose of this column to dispel myths and address these concerns among parents.
HPV is the most common sexually transmitted disease (STD) in the United States. It is estimated that nearly all sexually active Americans will at some point become infected with the virus. HPV is spread by direct skin to skin contact. Although the infection maybe asymptomatic, it is still possible to spread the virus. Condoms are not 100% effective to prevent HPV because infected skin may be present outside of the barrier.
Studies have demonstrated that 90 percent of sexually active males and 80 percent of sexually active females will be infected with HPV in their lifetime. Moreover, 50 percent of HPV infections are high-risk, which can lead to cancer if the body does not clear these infections.
HPV is a family of viruses that primarily produce warts, but a limited number are responsible for cancers. There are a total 120 different subtypes of the virus capable of producing warts on skin or mucus membranes. Specific strains of the virus show preference for sites of infection, and different disease progressions. For example, most types are responsible for common warts on the hands and feet, however, there are strains with a preference for producing genital/anal disease. Moreover, the HPV causing the most of significant concern are those strains responsible for certain cancers. Some HPV strains will directly interrupt a cells repair cycle, resulting in vulnerability to be transformed into a cancerous cell. HPV types 16 and 18 are high risk for cancer and account for 70% of all 490,000 cases cervical cancer with 3,900 deaths. In addition, these two types cause penile, anal and head/neck cancers.
Prevention is paramount because once infected there is no treatment for HPV infections. Only the associated lesions, including genital warts, recurrent respiratory papillomatosis (RRP), pre-cancers, and cancers are treated. Treatment options professionals utilize are biopsy, cauterization, cryotherapy, and can be mildly to severely disfiguring. Biopsy results are used to determine the HPV strain and treatment. High risk subtypes lead to increased medical observation and have the potential for more invasive treatments which can impair fertility and cause facial disfigurement.
The most popular HPV vaccine available for use is Gardasil. It has been proven to safely protect against HPV 16 and 18, which account for 70% of all cervical cancers. Gardasil additionally protects against other high and low risk virus types.
The Gardasil vaccine was initially developed in the mid 1980’s at various institutions in the US and abroad. HPV proteins were added to a previous vaccine base that was proved safe and effective. After almost 30 years of testing and scrutiny by the FDA, Gardasil was deemed safe and released to the public in 2006.
Since distribution of the Gardasil vaccine, 270 million were administered worldwide with less than .032% serious adverse events. The reported vaccine reactions are injection site discomfort, dizziness, and fainting. Furthermore, research has concluded that there is no association with neurological conditions such as Guillain-Barre’ and Autism.
Gardasil is licensed for use for males and females ages 9 through 26 years. The vaccines are administered in a series of three on a 0, 2, and 6-month schedule. Studies have shown vaccination earlier in the recommended age spectrum has more advantageous results. For example, vaccinated children between the ages of 9-11 display an almost 100% prevention of disease. Sexually activity is not a contraindication to receiving the vaccine, but the vaccine is not recommended to those currently pregnant.
Despite the safety and efficacy of the vaccines, one reason reported by parents for not vaccinating their children is the concern that vaccination will increase sexual activity in adolescents. Although disconcerting for parents, a study conducted two years before the introduction of Gardasil by the U.S. Department of Health and Human Services reported that the number of sexually active teens has increased to 30% in ages 15 to 17 and more than 63% in ages 18 to 19. Furthermore, these numbers continued to increase regardless of public programs in sexual education and abstinence.
Since released in 2006, Gardasil has made a direct impact on HPV prevalence in adolescents. Even with less than desirable vaccination rates, HPV prevalence among adolescent females age 14-19 is declining. The decline in affected teens is predicted to lead to decreased future HPV related cancers. These vaccinations are safe, effective, powerful tools at our disposal to protect our children from the detrimental effects of a preventable disease. If you would like more information on Gardasil, consult your local Family Physician, Pediatrician, or Obstetrician-gynecologists (OB/GYN). Remember the advice of CHOP pediatrician, Dr. Paul Offit regarding the HPV vaccination for adolescents, “it is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
Sources: CDC, Journal of Pediatrics, JAMA, International Journal of Cancer, Journal of Infectious Disease; www.MerckVaccines.com (GardasilR)
Medical Reviewer & Contributor: Anders Nelson, MD., F.A.A.P. is a pediatrician with offices in Scranton, PA.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Several years ago, while hiking to the bottom of the Grand Canyon with my family, my wife Esther developed “canyon knee,” also known as “hiker’s knee” or in medical terms, “patellar tendonitis.” Regardless of the term, the end result was that she had severe pain in the tendon below her knee cap and was unable to walk up the trail to get out of the canyon. In addition to ice, rest, bracing, and non-steroidal anti inflammatory medications, the National Park Ranger insisted that she use two trekking poles on her ascent to the rim.
Prior to that experience, I always thought that “walking, hiking sticks or trekking poles” were for show or those in need of a walking aide. Well, I could not have been more incorrect. Needless to say, Esther made it out of the canyon safely and, with the use of our life saving trekking poles; we have lived “happily ever after!” Now, 15 years later, I rarely walk more than 5 miles without my poles.
As a result of this experience, I have been recommending walking or trekking poles to my patients. These poles are an essential part of hiking or distance walking gear, for the novice and expert alike. Specifically, for those over 50 who have degenerative arthritis and pain in their lower back, hips, knees, ankles or feet, these simple devices have been shown to improve the efficiency of the exercise and lessen the impact on the spine and lower extremities. Additionally, using poles reduces the likelihood of ankle sprains and falls during walking. Trekking poles are also a safe option for those with compromised balance. If you want to walk distances for exercise and need a little stability but don’t want the stigma of a cane, trekking poles are for you.
Early explorers, Europeans and Native Americans have been using walking sticks for centuries. More recently, in the 1968 classic hiker’s bible, “The Complete Walker,” Colin Fletcher praised his “walking staff” for its multipurpose use: for balance and assistance with walking and climbing, protection from rattlesnakes, and for use as a fishing rod. Today, these sticks are now versatile poles made from light-weight materials.
Trekking poles are made of light-weight aluminum and vary in cost and quality. But, like most things, “you get what you pay for!” These hollow tubes can telescope to fit any person and collapse to pack in luggage for travel. Better poles offer multiple removable tips for various uses, conditions and terrains. For example, abasket to prevent sinking too deeply in snow, mud or sand; a blunt rubber tip for hard surfaces like asphalt or concrete, or the pointed metal tip to grip ice or hard dirt/gravel. Better quality poles offer an ergonomic hand grip and strap and a spring system to absorb shock through your hands, wrists and arms upon impact.

The poles should be properly adjusted to fit each individual. When your hand is griping the handle the elbow should be at a 90 degree angle. Proper use is simple; just walk with a normal gait pattern of opposite arm and leg swing. For example, left leg and right arm/pole swings forward to plant while the left arm/pole remain behind with the right leg .
This pattern is reciprocated with as normal gait advances (opposite arm and leg). I have been very pleased with my moderately priced poles (Cascade Mountain Tech from Dick’s Sporting Goods ($34.99 per pole). Prices range from $19.99 to 79.95 per pole. dickssportinggoods.com; montem.com; leki.com; rei.com. However, if you travel frequently to hike the State and National Parks, you may want to purchase more expensive poles that collapse and retighten more efficiently. (montem.com; leki.com;)
Montem Trekking Poles - with close-up of easy adjustable locking clasp.

There are numerous studies to support the use of trekking poles, especially research that supports their use for health and safety. One study compared hikers in 3 different conditions; no backpack, a pack with 15% body weight and a pack with 30% body weight. Biomechanical analysis was performed blindly on the three groups and a significant reduction in forces on lower extremity joints (hip, knee, and ankle) was noted for all three groups when using poles compared to those not using poles.
Another study confirmed that trekking poles reduced the incidence of ankle fractures through improved balance and stability. Additional studies support the theory that trekking poles reduce exercise induced muscle soreness from hiking or walking steep terrain and another study found that while less energy is expended in the lower body muscles using poles, increase energy is used in the upper body; therefore, the net caloric expenditure is equal as it is simply transferred from the legs to the arms.
In conclusion, it is important to remember that trekking poles for hiking or distance walking are much more than a style statement. They are proven to be an invaluable tool for health, safety and wellness by reducing lower extremity joint stress, improving stability and balance, and enhancing efficiency for muscle recovery.
Sources: Medicine and Science in Sports and Exercise. The Complete Walker, by Colin Fletcher
Model: Andrea Molitoris, PT, DPT at Mackarey Physical Therapy
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
It is four months since many people have made their health and fitness resolutions and hopefully some have stayed the course. If you are looking for another reason to stick to your New Year’s Resolution to get fit and lose weight in 2024 try this…to improve or prevent hip and knee pain!
There are three major weight-bearing joints in the body, the hip, knee and ankle/foot. Consequently, wear and tear and arthritis are common among these joints. There are almost 800,000 knee replacements and 450,000 hip replacements annually in the United States alone. While there are many recommended methods to avoid or delay joint replacement, only a few are within our control. Genetics, trauma, degenerative diseases such as rheumatoid arthritis and osteoarthritis are difficult to control. However, body weight, aggressive weight bearing sports and overdoing exercises as you age like excessive running, jumping, lifting and squatting can be modified or eliminated to limit the progression of joint damage. According to WebMD, “your knees are powerhouses. They’re the biggest, strongest, joints in your body, and most people use them throughout the day to sit, stand, walk, jump, and bend. They bear 80% of your body weight when you stand still and 150% or more when you walk across the room. In a 160-pound person, that’s 240 pounds of force!”
According to the National Institutes of Health, body weight or body mass index (BMI) has a direct impact on hip and knee degeneration, pain and dysfunction. In fact, one study found that people with or at risk of significant hip/knee osteoarthritis had a 2-3% reduction in risk of hip or knee replacement for every 1% reduction in weight, regardless of the baseline BMI.
It is commonly known that the primary cause of osteoarthritis is normal wear and tear, especially for those over 50. However, extra body weight can accelerate this process. As the joint degenerates, the cartilage at the end and in between your joints gets compressed and dehydrated which leads to deterioration. Eventually, the bones rub directly on each other as the cushion wears away, leading to pain, swelling, and stiffness, loss of motion, strength and function.
While it may seem obvious that extra weight will put more strain and stress on the hip and knee joints; another mechanism involved in this degenerative process. Excess body fat can increase chemicals in your blood stream that can cause inflammation in your joints.
If you need a goal and a motive, how about this: losing even 10 pounds will equate to 40 pounds less force compressing and stressing your hips and knees. Moreover, reducing body fat will limit the hormones that cause inflammation in your joints. Talk to your primary care physician or visit www.cdc .gov to find a BMI calculator. Just plug in your height and weight and it calculates it for you. For example, a 155-pound male at 5 feet 8 inches tall has a BMI of 23.6. (A BMI of 18.5 to 24.9 is considered a healthy weight for this person).
The Mediterranean Diet is a solid start to eating healthy. It is less of a diet and more of a lifestyle. The foundation of this diet is plant foods built around vegetables, fruits, herbs, nuts, beans and whole grains. Moderate amounts of fish, dairy, poultry and eggs with limited consumption of red meat are paramount. The Mediterranean lifestyle also includes shared meals with family and friends, small portions, regular exercise, and wine in moderation with food and friends.
Exercise has many more benefits than just losing weight. Physical activity is one of the most important factors in improving a lifestyle in a positive way. A minimum of 30 minutes of physical activity, 5 days per week can greatly contribute to weight loss and longevity.
Researchers have found that the benefits of regular physical activity are numerous. Some of the more important benefits are:
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well
SOURCES: WebMD, National Institutes of Health; CDC, American Council on Exercise
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
In addition to lowering blood pressure, this gentle form of exercise can help maintain strength, balance, flexibility and mental health and is an ideal activity for all ages!
This research was brought to my attention by my friend and mentor from Dalton, Peter Frieder, Chairman,Gentex Corporation and current Board Chair at WVIA. Peter is celebrating his birthday today with a number of years that clearly does not represent his physiological age, in great part due to his dedication to health and wellness. Happy Birthday and thank you!
According to a new study by the China Academy of Chinese Medical Sciences (CACMS), the ancient martial art practice of Tai Chi is effective in lowering blood pressure as much, if not more, than traditional aerobic exercise. For those with prehypertension or hypertension and are unable to tolerate the repetitive and prolonged weight bearing stresses of running, walking or cycling, these results have tremendous implications. The slow, gentle and controlled movements and positions of Tai Chi coupled with controlled breathing and meditation may be a valuable alternative, especially for those with aging muscles and joints. Improved strength, flexibility balance, posture and mental health are additional bonuses.
Tai Chi is multifaceted in that it combines martial arts, slow gentle and controlled movements, sustained postures, a focused and meditative mind, and controlled breathing. It is considered by many to be “meditation or medication in motion.”
Tai Chi involves slow-motion movements transitioning with control from one position to another. The positions have historically been named for the actions of animals, for example:

Deep and purposeful breathing, mental focus, body awareness and meditation are integral components of the exercise. The beauty of Tai Chi is not only in the physical form, but also in its safety for all levels of fitness. It is helpful for individuals from high level athletes to those with physical disabilities. The movements are natural and gentle without forcing the muscles and joints to extreme or uncomfortable positions. It is often used as an adjunct therapy in the wellness as well as rehabilitation of a variety of athletic (ACL surgery, joint replacements) and neurological conditions (Parkinson’s, MS, head trauma), to name a few. Based on the aforementioned Chinese study, Tia Chi can be applied as a technique to control or lower blood pressure, especially for those who cannot utilize traditional aerobic exercise.
Tai Chi has been found to offer many physical and mental benefits. Some of these include:
Muscle Strength – upper and lower body, trunk and core strength
Flexibility – participants report improved range of motion and flexibility of the spine and extremities
Balance and Proprioception – some studies report a reduction of falls due to a variety of sustained positionsand improved awareness of one’s body in space
Aerobic Conditioning - recent studies have found that participants have lower heart rate and blood pressure
Mental Health – through improved balance, strength, and flexibility, studies show participants have gained confidence and control as well as lower blood pressure and stress reduction.
All Tai Chi classes begin with four basic principles: warm-up, instruction, practice and breathing.
Warm-up- gentle easy motions to warm-up and loosen the joints and muscles to prevent injury.
Tai Chi Forms – “Short Forms” are beginner movements which are gentle, slow, and short in duration while “Long Forms” are more advanced.
Breath Work – gentle breathing combined with movement to relax the mind and focus energy
Don’t be intimidated by the language or history – Yang, Wu, Cheng are only brands of movements with a history of martial arts but this in no way impacts participation.
Get medical clearance – check with your physician to see if Tai Chi is safe for you. Some orthopedic or vestibular problems might require special attention.
Observe or take a beginner class – often available at local fitness clubs or senior centers. Research options in your area and find a friend to join you. Consider an introductory instructional video to get a feel for Tai Chi. (See local Tia Chi classes below)
Meet with an instructor – if it makes you more comfortable, make time to talk to an instructor before enrolling in a class.
Dress for success – wear loose-fitting clothes that allow for range of motion and comfortable shoes for balance and support.
Track your progress – use an app or keep a journal of your progress. Heart rate, blood pressure and endurance (the time you can hold a pose or tolerate a class) are easy to monitor.
Model: Lily Smith, University of Scranton Physical Therapy Student and PT aide at Mackarey Physical Therapy.
Sources: HarvardHealthPublishing; New Atlas; China Academy of Chinese Medical Sciences (CACMS); National Institutes of Health
Local Tai Chi Classes: Steamtown Yoga, Scranton, PA; Mission Yoga, Scranton, PA;Dragon’s Heart Tai Chi & Kung Fu, Clarks Summit, PA; Rothrocks Kung Fu & Tai Chi, Duryea, PA
For more information: HarvardHealth; www.taichihealth.com; www.treeoflifetaichi.com
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
Seasonal allergies affect 30 % of adults and 40% of children in the United States. Avoiding the outdoors is often not an option…especially if you enjoy outdoor activities and sports. Not long ago, it was unthinkable that an athlete with serious seasonal allergies could compete at a high level, such as the Olympics. Now, in great part due to advanced research, medications and proper management, an Olympic gold medal for those suffering from seasonal allergies is a reality. Recently, the National Institute of Allergy and Infectious Disease at the National Institutes of Health have published research on this topic to provide a better understanding and make recommendations.
The most common allergic reactions which athletes suffer from are sneezing, itchy and watery eyes, runny nose and coughing. Moreover, 67% of those with these symptoms also suffer from asthma. The athlete in NEPA is particularly vulnerable when the pollen count is high during spring and fall for several reasons. One, after being indoors all winter, one might develop a heightened sensitivity to allergens. Also, increased rapid and deep breathing during exercise makes athletes more susceptible to significant symptoms when exposed to allergens such as tree, grass and weed pollens.
Allergy skin testing can be performed to determine the allergens to which you are susceptible. Once determined, allergy shots are effective in building up tolerance to these allergens. If appropriate, you may be able to use allergy drops, administered under the tongue and conveniently used at home.
Asthma suffers should use their inhaler BEFORE symptoms occur. A recent study found that pretreatment using a short-acting bronchodilator inhaler within 15 minutes before exercise is very effective in preventing asthma symptoms for more than four hours. It is important to keep a bronchodilator available. If you fail to benefit from this, see your physician for other methods to control your exercise-induced symptoms.
Whether you have allergic respiratory problems from rhinitis or asthma, you many benefit from conditioning your airways with a 10 to 15 minute warm-up before and cool-down after the activity. This may serve to gradually prepare your lungs for an increased demand.
In addition to preventing dehydration on hot and humid days, constant hydration is very important for the athlete with allergies to prevent dry airways in athletes.
Know the signs and symptoms of asthma (coughing, wheezing, tightness in chest, shortness of breath).
Some schools have a file on each student athlete with a allergic or asthmatic problem which requires medication. The file includes information such as medical doctor release and instruction, emergency contacts and medications. Students must have their medications on hand before they can enter the field. The National Athletic Trainers Association recommends using a peak flow meter to monitor at risk players and can determine when a player can return to the field.
If possible, find an alternate practice facility with climate control for athletes at risk. Plan practices for these athletes when the pollen count is low. Check the newspaper or internet for pollen counts in your area. Training by the water, (ocean) where there is a breeze and less pollen is helpful.
Shower and change clothing immediately after being outdoors
During a flare up, do less aerobic exercise to limit stress on respiratory system. Try strength training indoors instead.
When pollen count is high, keep windows shut at home and in your car….use air-conditioning.
Keep pets out of your bedroom…especially when sleeping
Dry clothing in dryer…do not hang on clothesline outdoors
Sources: American College of Allergy, Asthma, and Immunology. National Athletic Trainers Association.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is dedicated to the memory of John R. O’Brien, Esq., who recently passed due to medical complications associated with multiple sclerosis (MS). John was a source of joy and inspiration for those fortunate to have known him. Twenty years ago, John hesitantly agreed to contribute to my column on MS with two requirements: one, if the column would be valuable to those affected by MS and two, he would remain anonymous. When speaking with his dedicated wife, Sally, it became very apparent that any discussion of John’s life would be diminished if it was defined by the disease because he was committed to turning his “DISABILITY INTO AN ABILITY!”
With the help of his loving wife, family, friends, and devices such as an electric scooter and adaptive car, John not only lived but thrived! He was a skilled lawyer, a respected member of the Bar, and an active member of the community. John served on the executive committee of the Lackawanna Bar Association. In addition, the Lackawanna Pro Bono honored him recently. He also taught business law and healthcare law and coached Prep’s mock trial team.
John shared his thoughts with me about the challenges of redefining life… from Golf Club Champion to living with a physically disabling disease. Anyone who knew him would agree that he succeeded in doing so through his keen intellect and sharp wit and humor…his heart and brain overcompensated for his body! In addition to reading books in Latin and Greek, he had his crossword puzzles published in The New York Times and Los Angeles Times. In September 2023, John conducted an interview with presidential historian Doris Kearns Goodwin before a full house at the Scranton Cultural Center. Ms. Goodwin later reported that John was the most knowledgeable, effective and enjoyable interviewer she’s encountered.
John’s absence will be deeply felt and his legacy will continue to shape our community for years to come!
Multiple Sclerosis is a chronic disease. While it may lay dormant and stable for a period of time, living a healthy lifestyle will make a positive contribution toward how you and your family live with Multiple Sclerosis. Studies show that a life of family, love, and support are essential to maintain a positive attitude with a chronic illness. This combined with a healthy diet and proper exercise can contribute greatly toward taking control and living a relatively normal life with MS.
As I have mentioned in many other columns, studies show that people with good attitudes and great faith live longer than others. This is especially helpful when living with chronic disease like Multiple Sclerosis. The Cleveland Clinic offers some suggestions how to maintain a positive attitude:
Many sources, including the Cleveland Clinic suggest that exercise, when performed properly, can have a positive impact on Multiple Sclerosis symptoms both physically and psychologically. However, because you have a chronic illness, you should consult with you family physician and physical therapist before beginning an exercise program. They will advise you on the proper type and amount of exercise.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
This column is dedicated to the memory of John R. O’Brien, Esq., who recently passed due to medical complications associated with multiple sclerosis (MS). John was a source of joy and inspiration for those fortunate to have known him. Twenty years ago, John hesitantly agreed to contribute to my column on MS with two requirements: one, if the column would be valuable to those affected by MS and two, he would remain anonymous. When speaking with his dedicated wife, Sally, it became very apparent that any discussion of John’s life would be diminished if it was defined by the disease because he was committed to turning his “DISABILITY INTO AN ABILITY!”
With the help of his loving wife, family, friends, and devices such as an electric scooter and adaptive car, John not only lived but thrived! He was a skilled lawyer, a respected member of the Bar, and an active member of the community. John served on the executive committee of the Lackawanna Bar Association and was recently honored by the Lackawanna Pro Bono. He also taught business law and healthcare law and coached Prep’s mock trial team.
John shared his thoughts with me about the challenges of redefining life… from Golf Club Champion to living with a physically disabling disease. Anyone who knew him would agree that he succeeded in doing so through his keen intellect and sharp wit and humor…his heart and brain overcompensated for his body! In addition to reading books in Latin and Greek, he had his crossword puzzles published in The New York Times and Los Angeles Times. In September 2023, John conducted an interview with presidential historian Doris Kearns Goodwin before a full house at the Scranton Cultural Center. Ms. Goodwin later reported that John was the most knowledgeable, effective and enjoyable interviewer she’s encountered.
John’s absence will be deeply felt and his legacy will continue to shape our community for years to come!
According to the National Multiple Sclerosis Society, Multiple Sclerosis affects approximately 400,000 people in the United States. Multiple Sclerosis is second only to trauma as the most common cause of neurological disability for those in early to middle adulthood. MS is almost three times as common in women. Multiple Sclerosis is very uncommon before adolescence or after 50. However, the risk increases from teen years to age 50.
Multiple sclerosis is considered to be an autoimmune disease. The immune system of the body does not work properly when it fails to attack and protect the body against substances foreign to the body such as bacteria. Instead, the system allows the body to attack normal tissues and create diseases such as MS, rheumatoid arthritis and lupus.
In MS, the immune system attacks the brain and spinal cord of the central nervous system. Each nerve has an outer covering of a fatty material (myelin) for insulation to improve the transmission and conductivity of impulses or messages to and from the brain. The damage to the myelin of the nervous system interrupts the ability of messages to travel to and from the brain, through the spinal cord and to other areas of the body such as the muscles in the arms and legs. Due to this “short circuiting” the brain becomes unable to send or receive messages. In multiple sclerosis, scar tissue or plaques (sclerosis) replaces the fatty myelin in “multiple” areas. This is also called demyelination.
The symptoms associated with MS vary greatly from person to person. The amount, frequency and speed of the demyelination process vary greatly and are directly related to the loss of strength and function in daily activities. Some people are independent and ambulatory with mild and infrequent episodes of weakness and disability and live a relatively normal life. Others suffer from frequent and aggressive episodes that significantly weaken and disable. Some common symptoms in the early stages include: muscle weakness, loss of coordination, blurred vision, pain in the eyes, double vision. Some common symptoms as the disease progresses are: muscle stiffness with muscle spasms, pain, difficulty controlling urination, difficulty thinking clearly.
The diagnosis of MS can be very difficulty in the early stages because the symptoms are often vague and temporary. Also, MS symptoms are very similar to other neurological problems. A neurologist will run several tests to rule out other possible problems. However, an MRI showing demyelination of the nerves is a primary confirmation.
Treatment for MS depends upon many factors and requires consultation with your physician. Some medications can control the frequency and severity of MS symptoms such as pain, weakness, and spasticity. Also, some drugs can slow the progression of certain types of MS. Additional treatments for MS include: diet, exercise, physical therapy, support groups, and counseling for the MS patient and their family. Part II of Multiple Sclerosis will discuss these options in further detail next week.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy - NEXT WEEK: PART II OF II - MULTIPLE SCLEROSIS
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
A myth is a traditional story, idea, or belief, especially one concerning early history of a people or explaining a natural or social phenomenon. It is a widely held but false belief or idea. In medicine, health myths are also widely held beliefs about health issues such as medicines, herbs, treatments, cures, antidotes, etc. which are partially or totally false and unsubstantiated in the scientific literature. This is a partial list of the most common health myths:
SOURCES: WebMd; National Institutes of Health, Mayo Clinic
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article does not intend as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
PEOPLE OFTEN ASK ME, “IS THERE SUCH A THING AS AN EXERCISE RUT?”. THEY WANT TO KNOW WHY THEY DO NOT SEEM TO BE IMPROVING WITH THEIR EXERCISE PROGRAM. They exercise 3-4 times a week for 30 to 45 minutes and they feel frustrated and STUCK in a rut.
The purpose of this column is to offer suggestions to improve or get more out of a “stale” exercise program. Last week’s column offered tips to improve a stale cardiovascular and strength program. We will discuss flexibility and functional training tips, including the components necessary for a healthy mind, body and spirit connection.
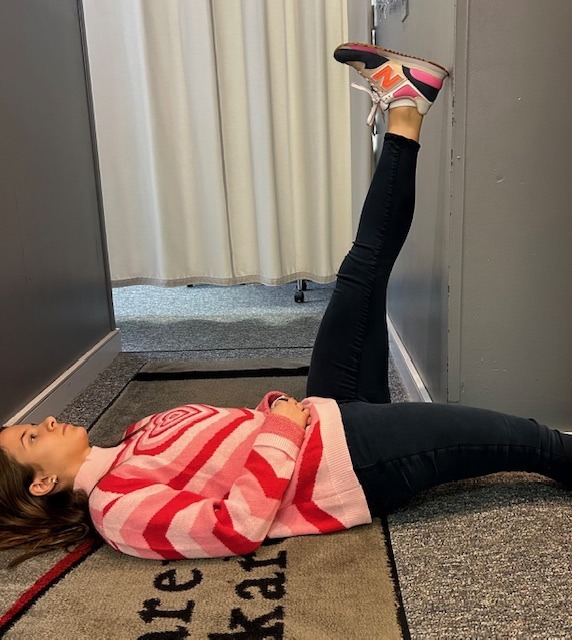
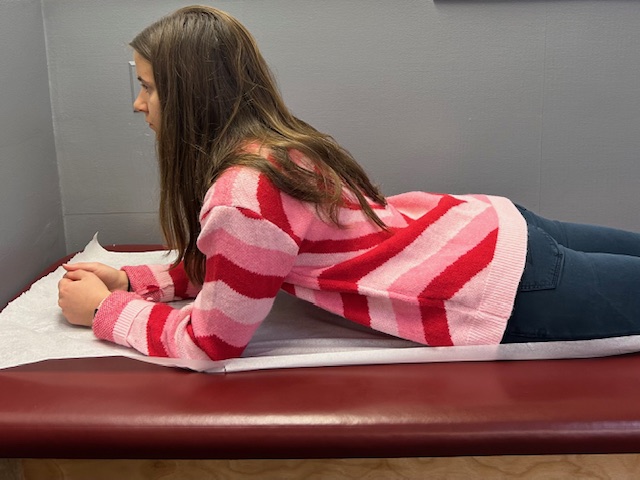
Flexibility training involves the careful stretching of the muscles, tendons and joints to improve range of motion in order to safely perform daily activities and sports without injuring or tearing soft tissues. It is probably the most neglected part of the fitness program. However, while the amount of inherent flexibility varies for each person, a minimal range is necessary as it relates to daily activities and sports. For example, as you age it is important to have enough flexibility in your back, hips and knees to wash your feet, put shoes and socks on. After a warm –up activity, perform flexibility exercises slowly and gently. There are two types of flexibility exercises; dynamic and static. Perform dynamic stretching with movement such as pushing the ankle up and down like a gas pedal. Complete passive stretching using an outside force, such as a towel to pull the ankle up to stretch the calf. Dynamic should be performed before an activity (before running or playing tennis) and static performed after the activity is over in order to increase range of motion for future activities.
In order to prevent an exercise program from getting stale, one must incorporate all aspects of wellness…a healthy mind, body and spirit!
It is easy for fitness enthusiasts to get so focused on maintaining a routine that they allow their program to become stale and ineffective. It is essential to reassess and update your program to prevent stagnation.
Make sure the routine has all three fundamental components of a well-balanced exercise program; cardiovascular, strength and flexibility training. Moreover, to be truly healthy, one must work toward a “Healthy Mind, Body, and Spirit. Therefore, in addition to traditional exercise one must incorporate the following: nutrition; meditation, relaxation techniques, yoga, core fitness; functional/sports specific training; leisure sports and activities
In order to prevent an exercise program from getting stale, one must incorporate all aspects of wellness…a healthy mind, body and spirit!
While each component offers its own specific benefit, the combination of all three cooperatively provides unique value. Too often, fitness enthusiasts concentrate on the exercises they LIKE or are good at more than the ones they NEED.
Sources: National Institutes of Health; American Council on Exercise
Model: Lily Smith, Physical Therapy Student, University of Scranton, PT aide, Mackarey Physical Therapy
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
PEOPLE WILL OFTEN ASK ME, “IS THERE SUCH A THING AS AN EXERCISE RUT?” THEY WANT TO KNOW WHY THEY DO NOT SEEM TO BE IMPROVING WITH THEIR EXERCISE PROGRAM…they exercise 3-4 times a week for 30 to 45 minutes and they feel frustrated and STUCK in a rut. While initially responding favorably to exercise, after 6 -9 months or more, they do not notice progress in weight loss, strength, tone, endurance or daily function.
The purpose of this column will be to offer suggestions on how to improve or get more out of a “stale” exercise program or an exercise rut. Step one is to build an exercise program that is grounded in the basics. Next step two, which begins after the basics have been mastered, includes the components necessary for a healthy mind, body and spirit connection and translates into functional activities of daily living including work and leisure sports.
Make sure your routine has all three fundamental components of a well-balanced exercise program; cardiovascular, strength and flexibility training. While each component offers its own specific benefit, the combination of all three cooperatively provides unique value. Too often, fitness enthusiasts concentrate on the exercises they LIKE or are good at more than the ones they NEED. A well-balanced program includes what you like and need! In fact, recent studies show that those performing all three components surpassed those performing one or any combination of two of the training types when tested for efficient oxygen uptake (VO2 Max), production of HDL (good cholesterol), lower body fat percentage, and lower blood glucose levels.
Cardiovascular exercise is any activity that raises your heart rate and respiratory rate. This type of exercise strengthens the heart muscle and the muscles that assist in breathing. When these muscles are stronger, they in turn work more efficiently to deliver oxygen to your muscles and other parts of the body. Ultimately, these oxygenated muscles can work harder and longer to burn fat during exercise and at rest.
Examples of Cardiovascular Exercises: Running, Brisk Walking, Swimming, Biking, Rowing, Elliptical Training and Stepper Training. Most experts recommend at least 30 minutes of sustained cardio, 3-4 days per week. However, recent studies support the notion of performing 10-15 minutes, twice daily, 4 days per week. For those “stuck” in a fitness or exercise rut, to advance your program, cardio should be performed 5-6 days per week for 45-60 minutes.
Strength training is an activity that provides any type of resistance to muscle contraction to build strength in the muscle. The resistance can be without movement against an immovable object such as pushing against a wall (isometric) or with movement such as lifting up or lowering a weight down against gravity (isotonic/dynamic). There are two types of isotonic muscle contraction; concentric, which involves raising the weight against gravity as the muscle shortens and eccentric which involves lowering a weight against gravity as the muscle lengthens. A standing biceps curl is an example that incorporates both concentric and eccentric contractions. A progressive strength training program includes all three types of muscle contraction. By using the classic bicep muscle curl these photos will demonstrate all three types of muscle contraction:
-Isometric Bicep Muscle Curl – pull up on door knob without allowing any movement of the arm.
-Concentric Bicep Muscle Curl – raise a dumbbell up against gravity as the muscle shortens.
-Eccentric Bicep Muscle Curl – lower a dumbbell slowly (4-6 seconds) against gravity as the muscle lengthens.
Sources: National Institutes of Health; American Council on Exercise
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
NEXT WEEK! Read Stuck in an Exercise Rut…Part II of II:
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!
