Happy 4th of July! As our country celebrates 250 years and the summer heat is kicking into gear, it is time to think about getting to the pool to cool off. It may also be time to think of your pleasure puddle in different light…a health spa! It may very well be the exercise of choice for many people. Many have discovered the benefits of moving their limbs in the warm water of a home pool following knee or shoulder surgery. Also, long distance runners who often look for cross training methods without joint compression and arthritis sufferers who are often limited in exercise choices by joint pain from compressive forces when bearing weight, can enjoy the buoyancy effects of water. These are good examples of the benefits or water exercise…aerobic and resistive exercise without joint compression.
Most doctors recommend some form of exercise with arthritis. Pain and fatigue are the most limiting factors for a person with arthritis. Pool exercise may be the answer. With proper technique, adequate rest periods, appropriate resistance and repetitions, water exercise can be very effective.
The following are some of the benefits of water exercise:
Visit your doctor regularly and listen to your body.

EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

According to the United States Environmental Protection Agency, NEPA and all of Pennsylvania is experiencing a change in climate as indicated by a half a degree (F) in temperature, more frequent and heavy rainstorms and the tidal portion of the Delaware River is rising one inch every eight years. Last summer was one of our hottest on record and this summer more is expected. For those without air conditioning or access to a lake or pool, it will also be remembered as record setting warm temperatures. A local reader who cares for her elderly mother wrote to express her concern about dehydration in the elderly. Age, diet, illness and medications are some of the many reasons why elders suffer from dehydration not only in the summer heat, but year-round.
Next to oxygen, water is the nutrient most needed for life. A person can live without food for a month, but most can survive only three to four days without water. Even though proper hydration is essential for health, water gets overlooked as one of the six basic nutrients. Dehydration occurs when the amount of water taken into the body is less than the amount that is being lost. Dehydration can happen very rapidly (i.e. in less than eight hours). The consequences can be life threatening and the symptoms can be alarmingly swift.
In the body, water is needed to regulate body temperature, carry nutrients, remove toxins and waste materials, and provide the medium in which all cellular chemical reactions take place. Fluid balance is vital for body functions. A significant decrease in the total amount of body fluids leads to dehydration. Fluids can be lost through the urine, skin, or lungs. Along with fluids, essential electrolytes, such as sodium and potassium, are also perilously depleted in a dehydrated individual.
Dehydration is the most common fluid and electrolyte disorder of frail elders, both in long term care facilities and in the community! Elders aged 85 to 99 years are six times more likely to be hospitalized for dehydration than those aged 65 to 69 years. More than 18% of those hospitalized for dehydration will die within 30 days, and associated mortality increases with age. Men appear to dehydrate more often than women and dehydration is often masked by other conditions.
Elderly individuals are at heightened risk for dehydration for several reasons. Compared to younger individuals, their regulatory system (i.e. kidneys and hormones) does not work as well and their bodies have lower water contents. Older adults often have a depressed thirst drive due to a decrease in a particular hormone. They do not feel thirsty when they are dehydrated. This is especially true in hot, humid weather, when they have a fever, are taking medications, or have vomiting or diarrhea. They have decreased taste, smell, and appetite which contribute to the muted perception of thirst. Because of dementia, depression, visual deficits, or motor impairments, elderly people may have difficulty getting fluids for themselves. Many elderly individuals limit their fluid intake in the belief that they will prevent incontinence and decrease the number of trips to the bathroom. The medications that they are taking (e.g. diuretics, laxatives, hypnotics) contribute to dehydration.
Elders may suffer headaches, fainting, disorientation, nausea, seizure, a stroke, or a heart attack as a result of dehydration. The minimum daily requirement to avoid dehydration is between 1,500 (6.34 cups) and 2,000 ml of fluid intake per day. Six to eight good-sized glasses of water a day should provide this amount. Better hydration improves well-being and medications work more effectively when an individual is properly hydrated.
Those who care for the elderly whether at home or in a health care facility need to be alert to the following symptoms:
By the way, plain old tap water is a good way to replenish fluid loss. Keep in mind that some energy drinks not only have excess and unneeded calories but also contain sugar that slows down the rate at which water can be absorbed from the stomach. Consuming alcoholic and caffeinated beverages actually have an opposite, diuretic effect!
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Crying is a normal and valuable part of human communication and emotional expression. No doubt, some use this form of expression more than others and being of Mediterranean descent, my family will tell you not to sit next to me in the movie theater if a “tearjerker” is playing. “The Notebook” really got me! While most people are not comfortable crying in public and may be viewed as a sign of weakness, current research shows that at appropriate times it may be healthy.
We cry for many reasons. Babies cry to communicate, adults cry when they are overwhelmed with positive emotions like a wedding, or negative emotions like a funeral. Crying too easily or too often can be a sign of an underlying emotional or physical problem. However, recent research has suggested that letting out a good cry at times of intense emotional build up, may be healthy.
Crying has intrigued scientists and medical professionals for centuries. Darwin, for example, purported that crying may have a role in evolution and natural selection. If tears can be a sign of emotional vulnerability and bonding, then it may keep communities together for the purpose of procreation.
According to research conducted by Dr. William Frey, humans may be the only species engineered to have such strong emotions that provokes the production of tears. Studies show that the fluid in a tear produced by emotion has a very different chemical makeup than the normal fluid that protects and lubricates the eye or the tears produced when peeling an onion. Recent research has found that a woman’s tears produced in response to sadness may counteract aggressive behavior in men. In the study, men were able to distinguish tears produced from a woman after watching a sad movie compared to saline tears by smell. Simultaneously, scans of the men’s brains while smelling the actual tears found decreased activity in areas of the brain associated with aggression.
Research on the health benefits of crying support the notion that a “good cry” is good for you. Nine out of 10 people report that after a “good cry” they feel better and are less stressful. The best thing about crying for good health is that it is free, almost everyone can do it, and except for a runny nose, red eyes, and runny mascara, it has no side effects. While not a miracle, some of the recent research suggests crying is highly effective at healing, and that it improves the mood of almost 90% of weepers, with less than 10% feeling worse. Some researchers go as far as suggesting that there may be a case for inducing crying in those who find it difficult to let go and cry, especially in people with clinical depression or mood disorders.
For some, the emotional build up prior to the cry was so stressful when trying to hold back the tears, crying served as a good emotional release. For others, while the emotional build up was stressful, the embarrassment of crying in public was more stressful. Overall, 60% of those who cried experienced a physiological response. The emotional buildup prior to the cry and the physical act of crying releases adrenaline to create a “flight or fight” response. This is immediately followed by a post-adrenaline period in which the person experiences physical and emotional release as the heart rate and blood pressure decrease when compared to the suppression of the cry.
Crying is a normal response to stress, emotional or physical trauma in both men and women. Not surprisingly, research has confirmed a long-held belief that those suffering from depression cry more than others. However, more concerning is the fact that those suffering from severe and debilitating depression with mood disorders have lost the ability to cry. Consequently, these individuals have lost the ability to derive the health benefits of crying such as the emotional release and physiological response. While both men and women cry equally when suffering from depressive mood disorders, men who are unable to cry tend to become more aggressive and irritable.
Crying is much more common among those suffering from a feeling of being overworked, overstressed and a loss of control. For these reasons, 71% of 3rd year medical students admitted to crying at least once in the past year. Among this group, most reported that crying was a valuable way of communicating and stress release.
So, the next time someone calls you a “cry baby” when you express your emotions by crying, tell them your “working out” by having a “good cry” to release stress, lower your heart rate and blood pressure and you don’t have time to go to the gym!
Source: Harvard Health Letter
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!


Gretchen graduated from Philadelphia College of Pharmacy and Science, The University of Scranton, and received a Doctor of Pharmacy degree from Temple University.
Gretchen has been teaching for over 25 years at Rutgers University, Keystone College, Lackawanna College, The University of Scranton, and Marywood University. She has earned certifications in Pilates, yoga, barre and teaches all three locally. She has a Wellness and Lifestyle coaching certification from Harvard University.
Gretchen resides in Scranton with her husband, Timothy Welby, MD, and has three daughters – Casey, Kate, and Caroline.
Lifestyle Medicine, is not just a fad or buzzword that is overused in a plethora of health, fitness and wellness magazines, but is actually a medical specialty. It is the practice of using diet and exercise, along with other lifestyle modifications to prevent and manage disease. Lifestyle Medicine focuses on six pillars: healthy eating, physical activity, restorative sleep, stress management, positive social connections, and avoidance of risky substances.
The American College of Lifestyle Medicine was established in 2004. Since then, its membership and outreach have grown exponentially. Lifestyle medicine is currently the fastest-growing specialty in medicine. Its primary aim is to utilize evidence-based therapeutic lifestyle interventions to prevent/control chronic diseases such as cardiovascular disease, type II diabetes, and obesity. However, new data is emerging which expands the role of Lifestyle Medicine into many other areas, including chronic low back pain, sleep, hormonal disorders, Alzheimer’s Disease, chronic inflammatory conditions, and mental health, to name a few.
Lifestyle Medicine differs from conventional medicine in that its approach is not disease specific. Following the six pillars of Lifestyle medicine improves overall health. Conventional medicine targets and treats a specific disease process with medication or surgical intervention in a reactionary approach. Lifestyle medicine prevents or reverses the disease process through behavioral and dietary changes. In a perfect world, Lifestyle medicine and Conventional medicine can be combined to achieve the best results for some patients.
A JAMA study, published in 1993, linked unhealthy lifestyles with premature death. Since this study was published, the rates of cardiovascular disease and Type II diabetes have continued to climb. Obesity rates are at an epidemic level. 70% of American adults, and 22% of children fall into overweight/obese Body Mass Index (BMI) categories. According to the American Academy of Cardiology, only 6.8% of adult Americans meet the criteria for ideal cardiometabolic health, something the Academy calls a “Population Level Code Blue.”
In 2020, the American Heart Association issued a Presidential Advisory for 2030 Impact Goals. The overall goal is to improve morbidity and mortality through preventative measures. Interventions should be targeted earlier in childhood and young adulthood, where healthy habits can be formed with greater success and maximum outcomes. For example, physical activity is well established for its positive effects on cardiovascular health. Physical activity prevents clot and plaque build-up, is antiarrhythmic, and provides hemodynamic stability. Physical activity has also been shown to have psychological, emotional, and social benefits. The American Heart Association categorizes physical activity as a Level 1 (highest) intervention for primary prevention.
Lifestyle Medicine is rooted in evidence-based findings, and its efficacy is supported in scientific literature. A study published in the New England Journal of Medicine in 2002 examined the prevention of the onset of Type II Diabetes in prediabetic patients. Patients were divided into three groups: a placebo group, a metformin group (a type 2 diabetes medication), and a lifestyle intervention group. The metformin group received daily metformin (medication intervention). The lifestyle intervention group received education and prescriptive interventions/instructions on diet, exercise, and stress reduction. Patients were followed for three years. At the end of the study period, the metformin group saw a 31% incidence reduction of type II diabetes, and the lifestyle intervention group saw a 58% incidence reduction in type II diabetes (almost double that of the medication group).
Many examples abound, highlighting the ability of lifestyle medicine interventions for healthy outcomes. The advantages of lifestyle medicine over conventional medicine interventions are numerous. Medications come with side effects. Medication costs are rising and are often not fully covered by insurance programs. Often, current medications are not completely effective for treating disease. For example, Alzheimer’s Disease treatments are lacking. The Alzheimer’s Association International Conference emphasizes healthy lifestyle interventions. They stress adopting 4 or 5 healthy lifestyle factors to reduce the risk of Alzheimer’s dementia by 60%.
Healthy eating habits do not lead to serious side effects. Lifestyle interventions are within the patients’ control and may result in cost savings, potentially lowering food and medical bills. Because lifestyle intervention involves behavioral changes, the process requires time and effort, as well as investment in education and reinforcement to sustain healthy patterns. Motivating clients to make necessary changes and stick with those changes can be the biggest challenge. A Lifestyle/Wellness Coach may be employed to start the client on their journey. The coach works with the client to make choices that are adaptable to the client while fitting within the six pillars. The role of the coach is to hold space and provide guidance for the client, but not to “fix”, “rescue,” or “judge”. Coaching sessions last 30-60 minutes. Coaches and clients may meet 10 times over 3-12 months to establish patterns.
If you, like so many others, have not achieved your health and wellness goals using traditional methods, it may be worth considering Lifestyle Medicine. Focus on healthy eating (minimizing processed foods and sugar intake), physical activity (minimum 300 minutes per week), restorative sleep (between 7-9 hours per night), stress management (controlling anxiety and depression), positive social connections (consistent interactions with friends) and avoidance of risky substances (alcohol, tobacco/nicotine, illicit drugs) have evidence-based positive outcomes to prevent, manage and reverse chronic diseases.
Sources: More information about the six pillars of Lifestyle Medicine and specific intervention outcomes can be found @Balanced Living 570 on Facebook and Instagram!
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Spring has finally arrived in NEPA as we get outdoors to enjoy sunshine and blue skies. It is also time to dust off your hiking shoes and hit the trails to enjoy fresh air and exercise…but don’t forget the trekking poles. I have been recommending walking or trekking poles to my patients for many years. These poles are an essential part of hiking or distance walking gear, for the novice and expert alike.
Specifically, for those over 50 who have degenerative arthritis and pain in their lower back, hips, knees, ankles or feet, these simple devices have been shown to improve the efficiency of the exercise and lessen the impact on the spine and lower extremities. Additionally, using poles reduces the likelihood of ankle sprains and falls during walking. Trekking poles are also a safe option for those with compromised balance. If you want to walk distances for exercise and need a little stability but don’t want the stigma of a cane, trekking poles are for you.
Early explorers, Europeans and Native Americans have been using walking sticks for centuries. More recently, in the 1968 classic hiker’s bible, “The Complete Walker,” Colin Fletcher praised his “walking staff” for its multipurpose use: for balance and assistance with walking and climbing, protection from rattlesnakes, and for use as a fishing rod. Today, these sticks are now versatile poles made from light-weight materials.
Trekking poles are made of light-weight aluminum and vary in cost and quality. But, like most things, “you get what you pay for!” These hollow tubes can telescope to fit any person and collapse to pack in luggage for travel. Better poles offer multiple removable tips for various uses, conditions and terrains. For example, a basket to prevent sinking too deeply in snow, mud or sand; a blunt rubber tip for hard surfaces like asphalt or concrete, or the pointed metal tip to grip ice or hard dirt/gravel. Better quality poles offer an ergonomic hand grip and strap and a spring system to absorb shock through your hands, wrists and arms upon impact.
The poles should be properly adjusted to fit each individual. When your hand is griping the handle the elbow should be at a 90 degree angle. Proper use is simple; just walk with a normal gait pattern of opposite arm and leg swing. For example, left leg and right arm/pole swings forward to plant while the left arm/pole remain behind with the right leg (PHOTO 1). This pattern is reciprocated with as normal=ait advances (opposite arm and leg). I have been very pleased with my moderately priced poles (Cascade Mountain Tech from Dick’s Sporting Goods ($34.99 per pole). Prices range from $19.99 to 79.95 per pole. dickssportinggoods.com; montem.com; leki.com; rei.com. However, if you travel frequently to hike the State and National Parks, you may want to purchase more expensive poles that collapse and retighten more efficiently. (montem.com; leki.com;)
There are numerous studies to support the use of trekking poles, especially research that supports their use for health and safety. One study compared hikers in 3 different conditions; no backpack, a pack with 15% body weight and a pack with 30% body weight. Biomechanical analysis was performed blindly on the three groups and a significant reduction in forces on lower extremity joints (hip, knee, and ankle) was noted for all three groups when using poles compared to those not using poles.
Another study confirmed that trekking poles reduced the incidence of ankle fractures through improved balance and stability. Additional studies support the theory that trekking poles reduce exercise induced muscle soreness from hiking or walking steep terrain and another study found that while less energy is expended in the lower body muscles using poles, increase energy is used in the upper body; therefore, the net caloric expenditure is equal as it is simply transferred from the legs to the arms.
Sources: Medicine and Science in Sports and Exercise. The Complete Walker, by Colin Fletcher
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

Allergies affect 30 % of adults and 40% of children in the United States. Avoiding the outdoors is often not an option…especially if you enjoy outdoor activities and sports. Not long ago, it was unthinkable that an athlete with serious allergies could compete at a high level, such as the Olympics. Now, in great part due to advanced research, medications and proper management, an Olympic gold medal for those suffering from allergies is a reality. Recently, the National Institute of Allergy and Infectious Disease at the National Institutes of Health have published research on this topic to provide a better understanding and make recommendations.
The most common allergic reactions which athletes suffer from are sneezing, itchy and watery eyes, runny nose and coughing. Moreover, 67% of those with these symptoms also suffer from asthma. The athlete in NEPA is particularly vulnerable when the pollen count is high during spring and fall for several reasons. One, after being indoors all winter, one might develop a heightened sensitivity to allergens. Also, increased rapid and deep breathing during exercise makes athletes more susceptible to significant symptoms when exposed to allergens such as tree, grass and weed pollens.
Sources: American College of Allergy, Asthma, and Immunology. National Athletic Trainers Association.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!


Guest Author: Andrea Molitoris Kozlowski, PT, DPT - Andrea is a doctor of physical therapy and an associate at Mackarey Physical Therapy in Scranton and Clarks Summit.
May is national pet month! As we take a moment to celebrate our pets it is important to acknowledge the many contributions having a pet brings to our lives, not the least of which is improving our health and wellness. Pets have a long history of helping humans navigate daily life. In fact, the oldest record of having a pet date back 15,800 years ago in Turkey where archaeologists found dog remains buried with humans.
Pets come in many different shapes, sizes, and species. Whether you are a cat/dog person, a reptilian lover, or marine life enthusiast, having a pet that is right for you can enrich you life in many ways. If you have never had a pet before or might be thinking about adopting a new addition to the house, it is important to research first and know the right ways to care for your new friend in the best way possible. Being a responsible pet owner will help to flourish your relationship with your pet and make the time and bond you share a stronger and more positive experience.
Making an informed and thoughtful decision about getting a pet is important. Don’t be afraid to ask questions, do some research, or simply take some time to figure out the logistics of how adding a pet can influence your life. From personal experience, I could not imagine my life without my four-legged friends by my side to share, enjoy, and enrich my every day. Having a pet can be one of the best parts of life. Remember, although having a pet can be a small part of your life; to them, you are their whole life, so make sure it can be the best life possible. Together, you will form of a bond that in enhances you life in many ways, including your health and wellness!
Sources: https://newsinhealth.nih.gov/2018/02/power-pets
Visit your doctor regularly and listen to your body. Keep moving, eat healthy foods, and exercise regularly.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

May is National Bike Month! For those who have a bike, now might be a good time to dust it off and enjoy the many beautiful and well-maintained trails that are available at the Countryside Conservancy at Lackawanna State Park, other locations in the Abingtons or the Lackawanna Heritage Valley Authority. For those who don’t have a bike, it might be a good time to get one!
However, whether you head out for 5 or 50 miles, ensuring a proper bike fit should be on your checklist. Riding a bicycle that is properly fit for your style and body will not only help to prevent injury but allow for a more comfortable riding experience. There are many things to take into consideration when checking your bike fit. First and foremost, you must choose a bike that fits your style of riding.
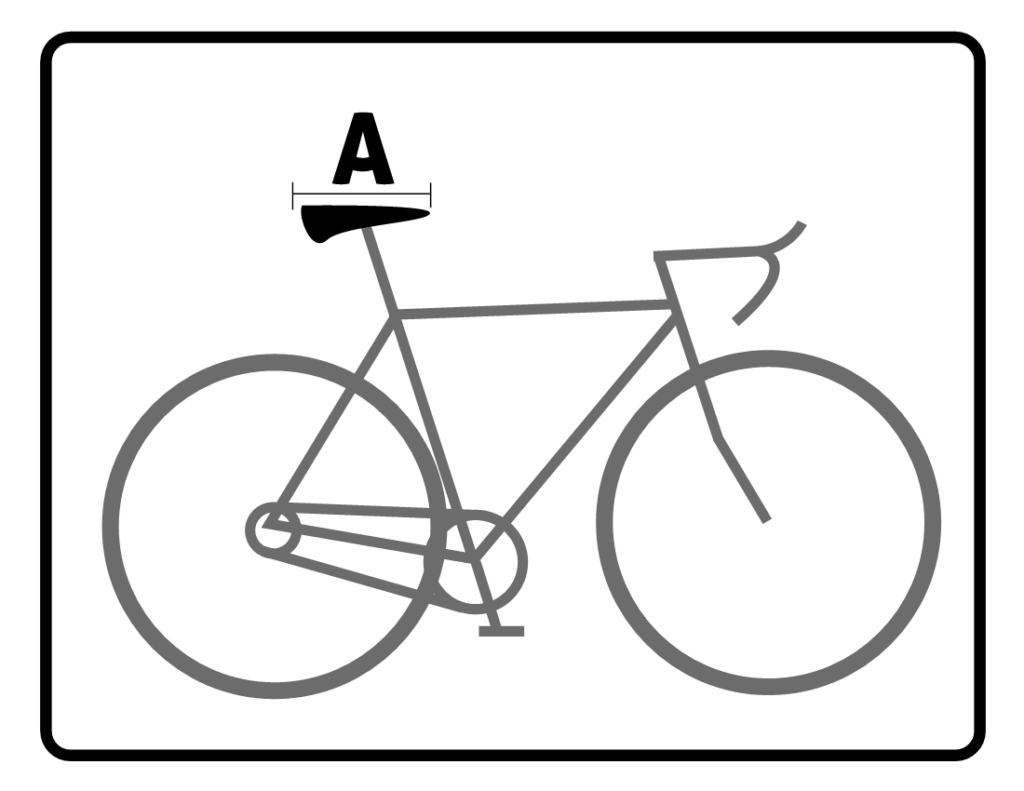
For the sake of simplicity 3 basic styles of bikes include Road bikes, Hybrid bikes and Mountain bikes. Road bikes are designed for long distance riders, hybrid bicycles can be used for longer distance riders, but usually accommodate a recreational cyclist, and mountain bikes are designed for dirt or gravel and technical trails. The next component of ensuring a proper bike fit is making sure that you have a good foundation by choosing the right sized frame. To find the right sized frame you can use the following guidelines as a way to start or simply ask the local bike shop or bike fit consultant of your choice for help.
Now that you have right size for your bike you should adjust the components of the bike to allow for a more comfortable riding experience. Please use the diagram as a point of reference for the following tips. Also be sure to re-examine your bike fit after any bad falls. Keep in mind these measurements are meant to be used as a simple guideline and if you have any preexisting injuries or concerns please be sure to consult your local Physical Therapist or bike fit consultant.
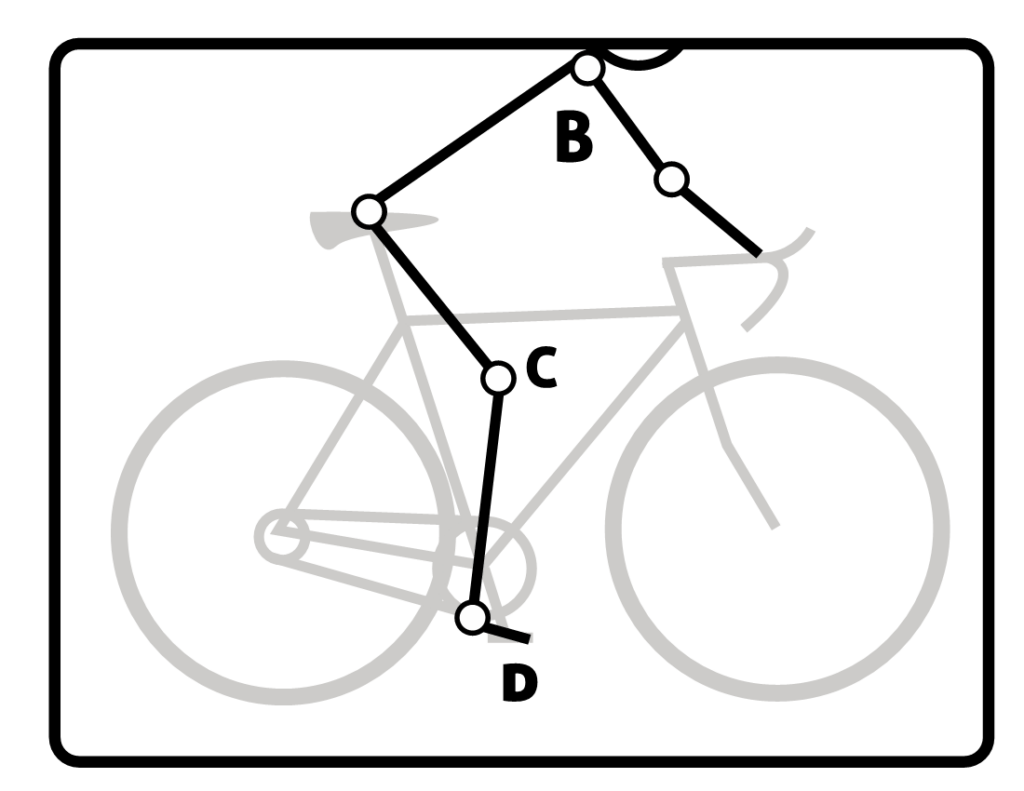
The knee to pedal measurement should be taken with the knee in the most extended position. There should be about a 25-35° angle at the knee (See “C” on diagram)
The ball of your foot should be over the pedal spindle (See “D” on diagram). This will allow for the best leverage, comfort and efficiency. Using a stiff soled shoe is recommended.
If you are a recreational cyclist, it’s a good idea to take all the proper steps in preventing injury. This article can be used as a reference point to help to prevent common cycling injuries, enhance your comfort and improve your riding efficiency. If you have any further questions about enhancing your bike fit, please contact your local physical therapist or bike fit consultant.
Sources: REI.com, APTA.org
Contributions & Illustrations: Sarah Singer, BFA, PTA
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

May is National Bike Month! It is time to dust it off your bike and enjoy the many beautiful and well-maintained trails that are available at the Countryside Conservancy at Lackawanna State Park, Lackawanna Heritage Valley Authority and other locations in the Greater Scranton Area. For those who don’t have a bike, it might be a good time to get one!
There are many obvious reasons to bike…cardiovascular fitness, burn calories, improve leg strength and others. But the real question is, “what are the advantages of biking over other forms of exercise?” Glad you asked…
Prevention is the best management of musculoskeletal problems associated with biking. First, many of the problems associated with biking such as knee pain, buttock soreness, and tendonitis can be prevented through proper fitting. Furthermore, it is important that your equipment be in good working order, such as tires, chain, brakes and pedals. Next, be sure to maintain a reasonable fitness level in order to bike safely. If you are a beginner, start slowly. Warm up and slowly bike for 10 to 15 minutes and build up over time.
Practice the coordination of stopping, starting, shifting and braking. Work on good strength and flexibility of the hamstrings, quadriceps, calves and gluteal muscles. All of these muscles are necessary to generate pedal force. Balance is also important to safety and can be practiced on and off the bike. Be aware that adaptive equipment can modify your bike for added comfort and safety such as soft handlebar tape, seat post and front fork shock absorbers, padded biking shorts, c-out and gel pad saddle seats, and wider tires.
Be careful not to progress too quickly because inactivity to over activity in a short period of time can create problems. Overuse injuries such as tendonitis can be avoided by cross training. Bike every other day and walk, run or swim on off days. Make sure to take time off to recover after a long ride. Use ice and massage to sore muscles and joints after riding.
Remember, cycling should be fun! Pain from improperly fitted and poorly maintained equipment is preventable. Excessive workouts and training rides should be kept to a minimum and consider cross-training in between.
EQUIPMENT: Helmets are a must! Also, keep your bike in good condition. Road bikes should have mirrors and reflectors. Use hand signals and obey traffic rules. Dress for weather and visibility. Have first-aid and tire patch kit, tire pump and tools. Seat comfort can be improved with gel cushion or split seat.
BE ALERT: for traffic, parked cars, pedestrians’ loose gravel and cracks in the road.
SOURCES: American Physical Therapy Association
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

“The woods are lovely, dark, and deep,
But I have promises to keep,
And miles to go before I sleep,
And miles to go before I sleep.” Robert Frost
On March 30, 2026, NEPA lost one of its most dedicated conservationists, Dorrance Reynolds Belin…our version of John Muir, Theodore Roosevelt, and Rachel Carson. While Dorrance served on numerous boards, in my view, he will be most fondly remembered for his environmental stewardship as founder of the Eastern Pennsylvania Chapter of the Nature Conservancy and Countryside Conservancy. I am not sure if Dorrance ever had the pleasure of meeting Robert Frost, Pulitzer Prize winning American Poet, but it is not hard to imagine that he had Dorrance in mind when writing the above poem. Thank you Dorrance, and those who worked with you, for the vision and foresight to preserve these special places for our children, grandchildren and great grandchildren to enjoy!
According to their mission statement, The Countryside Conservancy manages 1,190 acres of lands and waters to protect their conservations value. Most of these acres are open to the public for visitation and many have trails. Collectively, the conservancy contributes to 10 miles of singletrack hiking and biking trials to the 30-mile Lackawanna State Park/Countryside Conservancy Trail System …for more information visit: countrysideconservancy.org.
Please get outdoors and enjoy the trails…walking, running, biking, snowshoeing, cross-country skiing or horse back riding. But if you want to try something new this spring that will allow you to exercise on more interesting and less stressful surfaces in the beautiful woods of Northeast Pennsylvania…try trail running!
Trail running forces one to run 25% slower due to the uneven terrain (rocks, tree roots, stumps), incorporate “light running” techniques by running with short strides on the balls of my feet. You will feel much more refreshed by avoiding the direct sunlight under the cover of the trees. Furthermore, you can enjoy the up-close view of nature as I ran by cool streams and wet mossy rocks, beautiful flowers, rhododendron, and mountain laurel. Observe deer, chipmunks and birds. In my quest to avoid the hot sun, I discovered the beautiful underworld of “trail running” - it is beautiful, peaceful, natural and unique. It is fun to get in touch with your inner child as you run in the woods and get muddy. Trail running makes running fun…and it’s good for your joints!
The trail running community purports that trail running is popular because it satisfies a primal need for man to move through nature, derived from hunter/gatherer days. Others who promote trail running feel the popularity is due to the many advantages it offers. One, trail running prevents impact injuries due to soft surfaces. Two, the training style of running with shorter strides on the ball of the foot, lessens impact. Three, this type of running will develop stronger ankles and trunk core muscles while improving balance, coordination and proprioception from running on uneven surfaces. Lastly, the ability to release copious amounts of endorphins while breathing fresh air instead of roadside fumes is invaluable.
Find a Trail – Start by asking around. Hikers, mountain bikers, and horseback riders are a good start. The American Trail Running Association has a website with a free directory of trails in the United States. PA State Parks such as Lackawanna State Park in Dalton, offer many options www.visitPAparks.com, countrysideconservancy.org. or download the app AllTrails. Learn the difference between “nontechnical trails” which are wider with a paved, dirt or gravel base and much easier than “technical trails” which are narrow, rocky, hilly and challenging.
Sources: American Trail Running Association, Trailspace.com, countrysideconservancy.org.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” via Blog
EVERY SUNDAY in "The Sunday Times" - Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in hard copy
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopedic and sports physical therapy in Scranton and Clarks Summit. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine. For all of Dr. Mackarey's articles, visit our exercise forum!

