 Congratulations to the close to more than 2,000 runners who finished the 23rd Annual Steamtown Marathon yesterday. Most, if not all of you, are waking up this morning with a little less jump in your step than you had yesterday.
Congratulations to the close to more than 2,000 runners who finished the 23rd Annual Steamtown Marathon yesterday. Most, if not all of you, are waking up this morning with a little less jump in your step than you had yesterday.
Runners, by nature, are very active (often hyperactive) people who may have difficulty sitting and resting, even the day after a marathon. However, today should be a day of rest…you earned it! It is not wise to ignore the pain and stiffness in your muscles and joints. Therefore, I would like to offer some words of wisdom, based on science, to encourage you to adequately rest and allow your body to recover.
The Effects of Running 26.2 Miles on the Body:
(RunNow.com - Jim Peskett)
Muscle-Skeletal System:
One of the most obvious effects of running a marathon is significant muscle and joint pain and stiffness. It will set in after you sit for a while and attempt to get up and move around. For most, it will be more pronounced the day after the marathon, as you get out of bed and limp to the bathroom. Studies show that the leg muscles, (especially the calf muscles) display significant inflammation and necrosis (dead tissue) in the fibers of the muscle. In other words, the trauma to the muscles is so severe that tissue damage causes muscle cells to die. Consequently, studies found that muscle strength, power and endurance is compromised and required significant time to recover… sometimes as long as 4-6 weeks!
Additionally, many runners report severe bone and joint pain following the race. Some studies report findings of microfractures or bone bruising from the repeated and prolonged pounding of the marathon. It is purported that the stress on the joints may be related to: weight and body type, running shoes, running style and mechanics. While not dangerous, again, it is important to respect the stress placed on the body and allow adequate healing…LISTEN TO YOUR BODY!
Cellular Damage:
Creatine kinase is an enzyme found in the brain, skeletal muscles and heart. It is found in elevated levels in the presence of cellular damage to these tissues, for example, following a heart attack. Similarly, significantly elevated creatine kinase levels are found in the blood of runners up to 4 days post marathon, demonstrating extensive tissue damage at the cellular level. It is important to note, that these enzyme markers are present, even if a runner does not experience muscle soreness. So, adequate rest for healing and recovery is required, regardless of soreness.
Immune System:
It is not a coincidence that the runners are more likely to contract colds and flu after intensive training or running 26.2 miles. The immune system is severely compromised after a marathon and without adequate recovery; a runner can become ill and ultimately lose more training time or will underperform.
(www.runnersworld.com)
1. WALK
Once you cross the finish line, keep walking…for 10-15 minutes after the race to gradually lower your heart rate and prevent a buildup of lactic acid in your traumatized muscles.
2. EAT AND DRINK
Eat small snacks in the first hour after the race and avoid a big meal for later in the day and drink 24 oz. of water for every 2 pounds of weight loss after the race.
3. RELAX
If there was ever a time to enjoy a good movie or television show, it is after the marathon. Just get up and walk around every 20- 30 minutes.
4. ELEVATE YOUR LEGS
While relaxing, elevating your legs is a good idea to improve circulation. If your traveling by car or plane for longer than one hour, wear compression socks while you elevate.
5. ROLL AND MASSAGE
Wait approximately three hours after the race before you roll out and massage your muscles. Make sure you hydrate first.
6. STRETCH
Also wait 3 hours to gently stretch your tight muscles. Be gentle because the muscles are already traumatized.
7. DO NOT RUN
The research clearly states that running too soon will slow down full recovery. Many elite runners like Paula Radcliffe take one month off after the marathon and do yoga and cross-train.
8. WEEK ONE POST-RACE
No running. Do yoga, swim, walk, etc.
9. WEEK TWO POST-RACE
If you no longer have pain, continue cross-training and gradually introduce light, soft running for 30 to 60 minutes.
10. WEEK THREE POST-RACE
Gradually increase the time, distance and speed if you are pain free.
1. If I don’t have pain, then I did not damage my body and I can run again soon after the marathon.
FALSE: As stated above, enzyme levels that indicate cellular damage to the tissues are present in the post-marathon runner, even in those without significant pain.
2. Energy drinks with caffeine are the best way to reenergize my body and speed up my recovery.
FALSE: In addition to rest, drink, drink, drink - 24 ounces of water for every 2 pounds you lose after the marathon. This is based on pre and post exercise weight. You just burned 2,600 calories so avoid diet soft drinks. You need the glucose (sugar) boost. Also, don’t drink alcohol and use minimal amounts of caffeine (the equivalent of 1-2 cups of coffee). First, drink plenty of water and sports drinks (Gatorade) to prevent a diuretic like caffeine from messing up your fluid balance.
3. If I don’t run, I will lose all of my conditioning in one week.
FALSE: Studies clearly show that the VO2 Max, (the best measurement of a runner’s endurance and fitness), is unchanged after one week of inactivity. And, after two weeks, the loss is less than 6% and can be regained quickly. Moreover, it is important to remember, without adequate rest and recovery, performance is comprised, not by the loss of VO2 Max, but by muscle-skeletal tissue damage, which renders the leg muscles of the runner weaker.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
OVER THE COUNTER DRUGS…What You Need to Know
PART 2 of 2
(Read Part 1 here)
This is the second of two columns dedicated to the proper use of over-the-counter drugs used, especially during the “cold and flu” season. First and foremost, consumers must read and comprehend the information provided on the labels of all over-the-counter (OTC) medications before taking the drug themselves and before giving the drug to a loved one, especially a child.
According to the Centers for Disease Control, approximately 200,000 children (17 years old and younger), visit emergency departments each year due to adverse drug events, including OTC drugs, and children less than 5 years old are more vulnerable than older children. Dosing recommendations for this age group have not been established by the Food and Drug Administration. Many OTC remedies contain numerous ingredients which can increase the risk of an accidental overdose when using multiple products or when used in conjunction with prescription medication. Most product labels are vague about the hazardous consequences resulting when these drugs are given to infants and toddlers. There is no cure for the common cold and there is no evidence that OTC cold remedies are more effective than placebo in children under 2 years of age. The American Academy of Pediatrics recommends alternative solutions to alleviate the symptoms of a child’s cold: (1) To loosen mucous in the nose, use saline nose drops or a cold-air humidifier, (2) To clear nasal congestion, use a rubber suction bulb. If parents have patience and allow several days, the child’s symptoms usually subside. If your child frequently experiences a runny nose, earache, or sinus infection, food intolerances can be the culprit. Avoiding provoking foods such as dairy, wheat, corn, and tree nuts often affords relief to the child with food allergies.
“Pharming” is when teenager’s use prescription and OTC medications to get “high.” OTC cold remedies containing Dextromethorphan (DXM) are popular recreational drugs for children between the ages of 13 and 16 to induce the sensation of intoxication and even hallucinations. A survey conducted by the Partnership for a Drug-Free America concluded that 1 out of 11 teens has used OTC cold remedies for a recreational “high”. DXM is readily available (probably in your medicine cabinet), inexpensive, and not illegal. DXM is considered a “drug of concern” by the Drug Enforcement Agency but there are no legal restrictions except that OTC medications containing DXM are now stored behind the counters of retail stores .
DXM is an ingredient in more than 120 OTC cold remedies including: Robitussin, Nyquil, and Vicks Formula 44. Chemically similar to morphine, DXM has been added to cough syrups and cold medications since the 1970’s. Coricidin HBP Cough and Cold Tablets contain a significantly higher dose of DXM providing an easy and convenient “high” after the ingestion of only a few pills.
In addition to DXM, OTC diet pills, sleep aids (Tylenol PM, Excedrin PM, Sominex), and motion sickness medication (Dramamine) are also abused by teenagers. Diet pills have the potential to produce a “high” and Dramamine causes hallucinations when recommended dosages are exceeded. The abuse of sleep aids can result in narcolepsy. As the frequency of usage increases, teens are at risk of developing physical and psychological dependence to these drugs.
Today’s teens are more likely to abuse OTC medications because of the plethora of information available. Advertisements in magazines, newspapers and on the television have portrayed OTC drugs as safe or harmless. The internet provides an abundant supply of information to the computer savvy teen. Children have access to knowledge about what kinds of OTC remedies to buy for a “high” and exactly how much of the drug should produce the desired effect. The effects of OTC medications can be enhanced and potentially fatal when combined with other OTC drugs, alcohol, or prescription medications. Fortunately, many of these medications are now only available “behind-the-counter” and some states limit how much a person can purchase each month.
Children abuse drugs to gain social acceptance or to alleviate stress from school, friends, and family. Be alert for a child that may be abusing OTC drugs if drugs are missing, grades decline, behavior changes, or eating/sleeping is disrupted. Potential OTC drug abuse can be prevented by: conducting regular drug inventories, communicating with and listening to your children, and establishing well-defined family rules to provide your teen with the information necessary to give the appropriate responses when confronted with recreational OTC drug abuse. Contact your physician if you suspect a potential OTC abuse problem in your child or loved one.
CONTRIBUTIONS: Janet Caputo, PT, DPT, OCS
Read “Health and Exercise Forum” by Dr. Paul J. Mackarey every Monday in The Scranton Times-Tribune. Dr. Mackarey is a doctor of orthopedic and sports physical therapy with offices in downtown Scranton. Dr. Mackarey is an associate professor of clinical medicine at GCSOM.
OVER THE COUNTER DRUGS…What You Need to Know
PART 1 of 2
According to the Consumer Healthcare Products Association, approximately 3 billion trips to the pharmacy are made each year to purchase over-the-counter (OTC) drugs in the United States. The average household spends about $338. per year on these products and seven out of 10 parents have given their child an OTC in the middle of the night for various symptoms. Consumers purchase OTC remedies for a variety of ailments; to reduce fevers, ease body aches, soothe sore throats, and alleviate nausea and diarrhea. OTC medications are considered safe if they are used according to the directions printed on the label. However, there is much more to be considered when using these products.
OTC medications are readily available, are often less expensive than prescriptions and can be purchased without a visit to the physician’s office. The FDA considers these drugs to be safe for healthy consumers to use if the instructions printed on the label are followed. These medications have few side effects, low toxicity, and a low potential for abuse. Nonetheless, there is the possibility of serious and unpredictable interactions with other drugs that the consumer may be taking. Therefore, if the consumer is taking other prescription or OTC medications, a consultation with a doctor or pharmacist before selecting an OTC remedy may be a wise decision. Furthermore, the consumer must “self-diagnose” when using OTC medications which may result in mistaking a minor ailment for a more serious illness. For example, “headache” may indicate a brain tumor or “heartburn” may be a sign of a heart attack! Moreover, older individuals are at greater risk of developing adverse effects and drug interactions from OTC medications because increasing age affects the absorption, distribution, metabolism, and excretion of many drugs. Finally, some OTC drugs such as cold remedies, cough syrups, and pain killers contain substances that can produce drowsiness, impair judgment, and slow reaction times. Individuals experiencing these side effects are at risk of injury or even death while operating equipment or motor vehicles.
There are several other problems that can occur when using OTC medications. Even though the side effects of OTC drugs are few, they can be dangerous. Heart attacks and strokes can be side effects of Advil, Aleve, and Motrin which are classified as non-steroidal anti-inflammatory drugs (NSAIDs). An OTC remedy may worsen a pre-existing condition. NSAIDs can aggravate peptic ulcers and some decongestants can elevate blood pressure. Because OTC medications are mistaken as “harmless”, they are often taken more frequently and in higher dosages than recommended which can cause organ damage and toxicity. An accidental overdose can occur since some of the actions of OTC medications are similar to prescription drugs. For example, OTC aspirin taken with prescription Coumadin, Heparin, or Plavix can result in excessive thinning of the blood and increase the risk of bleeding. Rare and unpredictable allergic reactions can be produced by some OTC drugs. Anaphylaxis, a life-threatening allergic reaction, is a possibility after taking Aspirin or Advil. The consequences of the prolonged or excessive use of some OTC remedies can require years or decades to develop: liver and kidney damage or osteoporosis.
The consumer has the ability to alleviate the annoying symptoms associated with many common conditions through the use of OTC medications. However, the right to purchase OTC medications does not come without responsibility. In order for these drugs to be used safely, the consumer is advised to follow these guidelines: (1) Read the label for the active ingredient, correct dose, precautions, and which conditions would make the drug a poor choice. (2) Consult a pharmacist or physician when in doubt about which active ingredient would most appropriately address a particular symptom or to identify drug interactions and side effects. (3) Select an OTC drug that treats your exact symptoms. If you only have a cough, avoid the multi-symptom remedies. (4) OTC medications are intended for short-term use. Do not exceed the recommended treatment duration. If symptoms persist, consult a physician. (5) Consult a physician before taking any OTC remedy if you have health problems or are taking prescription medications. (6) Use reliable internet resources for more information such as WebMD or Epocrates Rx on iTunes App Store.
CONTRIBUTIONS: Janet Caputo, PT, DPT, OCS
Read “Health and Exercise Forum” by Dr. Paul J. Mackarey every Monday in The Scranton Times-Tribune. Next week read, Part II of II OTC Drug Safety. Dr. Mackarey is a doctor of orthopedic and sports physical therapy with offices in downtown Scranton. Dr. Mackarey is an associate professor of clinical medicine at GCSOM.

Patrick Connors, M.D.
Guest Author: Patrick Connors, MD, 2014 Graduate TCMC (GCSOM)
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine.
In 2009 65 young men and women became part of TCMC’s (now GCSOM) charter class and less than ten years later, after completing residencies in various medical specialties, 14 have return to NEPA to serve our community. Dr. Patrick Connors, class of 2014, is among those eager to contribute to the health and wellness of the people in his hometown. Dr. Connors, son of Pat and Ann Biglin Connors, graduated from Dunmore High School and Temple University before attending TCMC (GCSOM) school. He completed his residency in internal medicine at Thomas Jefferson University Hospitals in Philadelphia and is practicing at the Prime Med office on Pittston Avenue.
“It is nice to practice in an area with people who have meant so much to you,” says Dr. Patrick Connors, Dunmore native who has recently returned to NEPA to practice medicine with Prime Med in South Scranton. He is eager to give back to the community he feels gave him so much. In this column, Dr. Connors and his staff have compiled a list of suggestions that will make your visit to the doctor more effective and efficient.
The majority of visits with your doctor are scheduled to last about 15 minutes. Making the most out of such a short encounter is a challenge, but a little bit of preparation can go a long way. With many people only seeing their doctor once or twice per year, the importance of being prepared is enormous. The following is a list of tips to help you make the most out your 15 minutes.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commowealth School of Medicine.
HEALTH AND EXERCISE FORUM, By: Dr. Paul J. Mackarey
Compression Socks for Runners – Wear After The Race! Jury Out on Value for Running Performance –
But New Research Suggests Socks May Prevent Post Race Bloot Clots --One month to go until the Steamtown Marathon!
The 23rd Annual Steamtown Marathon will be held on Sunday October 7, 2018. Approximately 2,500 runners will attempt to conquer 26.2 miles from Forest City to downtown Scranton. While I have not participated in the event in several years, I would like to share some of my past running mistakes with the hope that you might have a better and healthier race and recovery…consider using compression socks AFTER you train/race if the run is longer than an hour and the drive/fight home is longer than 1 ½ hours.
Completing the long and arduous 26.2 mile journey is not an easy task. In fact, the mechanical and physiological toll on your body is tremendous; from painful joints, muscles, tendons, to black and blue toes. Not so obvious, however, is the damage to your deep veins and tissues of the circulatory system. New research indicates that strenuous endurance exercise, such as marathon running, stimulates the clotting mechanisms in your body in response to the multiple micro traumas sustained over 2 or more hours. While most healthy athletes will naturally heal from post exercise clot formation, others may be at risk…those traveling more than 1 hour (by car, bus, train or plane). The risk increases substantially for those with a longer period of travel/sitting post-race, history of previous trauma, blood clots or have the genetic predisposition for clot formation.
What Are Compression Socks? How Do They Work?
Compression socks are familiar to most people as the tight knee-high support stockings worn after a surgical procedure such as a knee or hip replacement to prevent blood clots. They are made with a special fabric and weave design to provide graduated compression (stronger compression at foot and ankle and less at the top of the sock) to promote better circulation and movement of fluids from the foot, ankle and calf back to the upper leg and ultimately the heart. Compression socks work similarly in runners. As the stagnant fluid with lactic acid and other byproducts of exercise is removed from the space, fresh blood, nutrients and oxygen is replaced to foster healing of micro damage to tissue and promote more efficient use of the muscles.
Is There Any Research?
The Journal of Strength and Conditioning Research published a study that found wearing compression socks improved running performance. However, similar studies have failed to support this claim. One finding that has been repeatedly supported in the literature, including The British Journal of Sports Medicine, found that compression socks worn in soccer players and runners improved the rate and magnitude of recovery. Moreover, recent studies, including a study with the Boston Marathon, have demonstrated the reduction in clotting mechanisms in those wearing compression socks AFTER the marathon, as compared with those wearing “sham” socks. Benefits seem to be less obvious for short duration activities or when running 10km or less.
Conclusion
In conclusion, only time will tell if compression socks will improve performance in runners will or be merely a fad based on placebo or true fact supported by scientific research. Based on current wisdom, these socks may offer value and benefit AFTER activities of long duration (more than 1 hour) or long distance running (more than 10km) to expedite the recovery from exercise-induced blood clot formation, muscle soreness from the accumulation of lactic acid and other muscle damage byproducts.
It is this author’s opinion that this product is worth a try. However, whenever you try something new for your sport, trials should occur during practice and if successful used during competition. Consider trying a lower compression to begin (the socks come in different degrees of compression). Even if one is hesitant to use the product while running, it appears the greatest value of the sock is after a prolonged training session or competition to reduce exercise-induced muscle soreness and prevent blood clots, especially in athletes at risk for clotting and those traveling for an hour or more after the race. Additionally, in view of the fact that some studies which showed only minimal to moderate improvement in well-trained athletes, it may be that those in greater need, such as deconditioned individuals attempting to begin a fitness program and novice weekend athletes, may benefit more from compression socks than elite athletes.
TAKE HOME: Runners, cyclists, triathletes, soccer players and others participating in endurance sports should consider compression socks, if not during the activity, certainly following the activity for 24 to 48 hours…especially those at risk for blood clots and those traveling for more than one hour after the race.
With one month to go before the Steamtown, it is not too late to try compression socks and see if they work for you during and more importantly, after your long training runs.
Where to find compression socks:
2XU Compression Racing Sock – www.2XU.com
Scranton Running Company – Olive Street - Scranton
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Since 1894 Labor Day has been designated as the national holiday that pays tribute to the contributions and achievements of American workers. Research supports the notion that healthier employees are happier and more productive. When employers encourage healthy behavior and safety at work, they benefit in many ways. For example, in addition to improving job satisfaction and productivity, healthy employees save money by using less sick time, worker’s compensation benefits and health benefits. For example, according to the Centers for Disease Control and Prevention, approximately 75 percent of employers” health care costs are related to chronic medical problems such as obesity, diabetes, high blood pressure, and high cholesterol. Deconditioned, overweight employees are more likely to suffer from these preventable conditions and are at greater risk for injury. Employers, please consider using this holiday as an opportunity to start a health promotion program at your workplace…have a health fair, offer healthy snacks, encourage walking, smoking cessation, exercising at lunch, and offer fitness club stipends.
Lower back pain, one of the most costly illnesses to employers, is one example of a problem which can be prevented with a good health and safety program. It is widely accepted in the medical community that the best treatment for lower back pain (LBP) is prevention. Keeping fit, (flexible and strong), practicing good posture, and using proper body mechanics are essential in the prevention of LBP. At our clinic, significant time and effort is spent emphasizing the importance of these concepts to our patients and employees.
The City of Scranton is a perfect example of the merit and value of LBP safety and prevention. I have served as a rehab consultant for the city, working with human resources and they have saved significant dollars in workers compensation dollars with a safety program. During this time, the city has noticed a significant reduction in LBP injuries through an onsite safety program which promotes education, wellness, body mechanics, lifting techniques, postural and stretching exercises and ergonomics.

Proper Sitting Technique
Perform postural exercises throughout the day. Most of the day we sit, stand, and reaching forward and bend our spine. These exercises are designed to stretch your back in the opposite direction of flexion. Please perform slowly, hold for 3-5 seconds and repeat 6 times each 6 times per day.
Good Body Mechanics and ergonomics are also important in the prevention of LBP. When lifting, think twice. Think about the weight, shape and size of the object. Think about where the object is going and the surface resistance of the floor. Does it require two people to lift? Can I safely lift that high or bend that low?
When bending to lift an object think about safety:

Proper Lifting Technique
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
ADDICTION: Avoiding Opioid Dependence and Alternatives to Pain Medications
Part 2 of 2
(read Part 1 of this series at this link)
International Overdose Awareness Day, August 31, 2018
Special Feature “ Health & Exercise Forum” with Geisinger Commonwealth School of Medicine the 3rd Monday of every month!
Guest Columnist: Anthony Morada, MD2

Anthony Morada, MD2
Anthony Morada, a second year medical student at Geisinger Commonwealth School of Medicine (GCSOM). Anthony Morada majored in Cell and Developmental Biology and minored in English at the University of California Santa Barbara. As a community advocate, Anthony has hosted a Metastatic Breast Cancer Symposium at GCSOM and will be hosting a free Hepatitis B Screening at GCSOM for the Steamtown Health Fair on September 22, 2018.
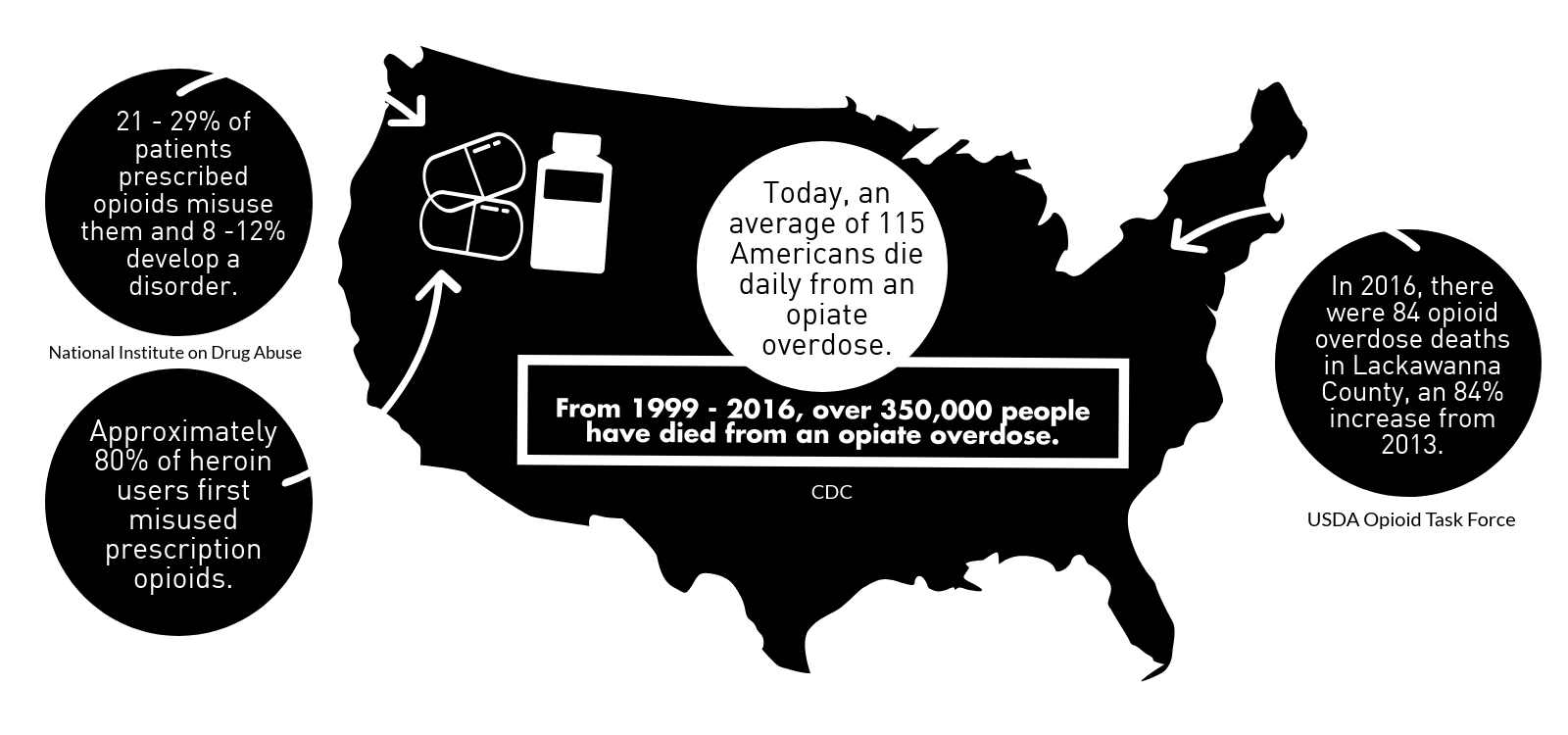
In 2017, Pennsylvania recorded the second highest increase in deaths from opioid overdose in the country.1 While this alarming measure included illegal opioids such as heroin, prescription painkillers consisted of more than 40% of all US opioid overdose deaths - calculating to more than 46 victims per day.2 Prescription painkillers like Methadone, Oxycodone, and Hydrocodone, are part of the opioid drug class because of the way they affect the pain receptors in the body. These pills are commonly prescribed by physicians to treat severe or persistent pain. While most patients appropriately use opioids to manage their pain, minimizing opioid use and seeing alternative forms of pain relief can help reduce the risk of opioid dependence and overdose.
Know The Risk Factors – Who is Most Vulnerable?
Eliminating the need for opioids completely or using the lowest needed dose will reduce the chance of developing opioid addiction disorders. Research found that among patients prescribed opioids for chronic pain, approximately 10% of them will be diagnosed with an opioid use disorder.3 As the name describes, patients with an opioid use disorder rely on or are addicted to opioids, including prescription drugs and heroin. While not all patients will experience reliance on these drugs, researchers identified factors that may be associated with an increased risk of developing an opioid use disorder: the presence of another substance use disorders (including tobacco use disorders), a family history of substance use disorder, other mental health disorders (such as depression or posttraumatic stress disorders), a history of legal problems or incarceration, and individuals using opioids younger than 40 years of age.4,5 Therefore, patients meeting any of the previous criteria should be aware of the increased risk for developing opioid use disorder. Consequently, opioid addiction parallels the increased risk of death primarily due to the elevated rates of overdose and trauma.
Limit Exposure and Opportunity
Eliminating prescription opioids in the household can minimize the chance of family or friends from getting possession of opioids. Investigators found that prescription opioids were more often obtained from friends or relatives than from a clinician.6 Therefore, by removing unnecessary opioids, patients can reduce the amount of drugs in the community. Fortunately Pennsylvania’s Department of Drug and Alcohol Programs has a Drug Take-Back Box Program that allows individuals to safely dispose of their unused opioids at their local hospitals and pharmacies. While complete elimination may not be entirely reasonable, taking the minimum dose needed or alternative non-opioid pain relief can yield similar outcomes while decreasing the chance of adverse events.
In response to the epidemic, the Centers for Disease Control and Prevention (CDC) released prescription guidelines that recognize specific situations where a low dosage of opioids are appropriate such as: cancer treatment, palliative care, end-of-life care, and certain acute care situations. For long term pain management, the CDC recommends physical therapy for symptoms that are related to low back pain, osteoarthritis, fibromyalgia, or other chronic pain lasting longer than 90 days.7 Research has found that, treatment with opioids was not superior to nonopioid treatment for improving pain-related function over 12 months. The American Physical Therapy Association’s (APTA) launched a national public awareness campaign to encourage patients to #ChoosePT as a safer alternatives for long term pain relief.
Find Safer Alternatives for Pain Management
As a more permanent solution, physical therapy breaks the cycle of chronic pain while opioids temporarily masks symptoms and actually delays recovery. A physical therapist will partner with their patient to create a customized plan of care that addresses their painful movement faults. Physical therapists can treat symptoms through therapeutic exercise, hands-on techniques, and patient education on chronic pain management.8 Exercise therapy can be modified to include aerobic, aquatic, and resistance exercises that addresses musculoskeletal imbalances or poor conditioning causing pain. Impairment-specific exercise programs combined with patient education on pain mechanisms can help address fear associated with chronic pain symptoms. Physical therapists can also address proper posture, ergonomics, sleep positioning, and body mechanics to decrease overall daily stress on the body and improve functional capacity.9 Patients can be referred to other experts on behavioral and stress management techniques that promote overall health and wellness. The education process includes building a multidisciplinary team and setting patient-centered goals that are realistic for recovery without opioid use.
Use Resources
Victims of an opioid use disorder have a number of resources to help them manage their disease, and reduce the risk of recurrence and overdose. While self-diagnosing an opioid use disorder may prove difficult, there are a number of signs that may suggest a misuse of prescription drugs - these indications include: using more drugs than planned or for a longer period of time, unable to cut down the need for drugs, having a craving or strong desire to use, neglecting work or family, or any other symptoms that prevent the individual from previously normal activities.10 Individuals who are worried that they may have a problem with drugs are highly encouraged to talk to their primary care physician, or a mental health counselor. This way consultation and treatment programs can begin before the drug abuse gets out of hand. Normally, treatment of opioid use disorders involves 3 components: medicine, counseling, and support groups. Physicians can prescribe medicines that help patients reduce drug cravings and eliminate the high that comes from opioids. Addiction counseling helps patients come to terms with their addiction and helps them develop a life that does not involve drugs.
While support groups, like Narcotics Anonymous, provides a forum for those with the same conditions to share their experiences and advice with each other. In Scranton, there a few local resources aimed to help those with opioid and other substance use disorders. Some of the example organizations are the Greater Scranton Steamtown Area of Narcotics Anonymous and the Drug and Alcohol Treatment Service, Inc. in Scranton. The Pennsylvania Department of Drug and Alcohol Programs also supports a 24 hour hotline with a purpose to assist patients in finding treatment providers or funding for addiction treatments; this number can be reached at 1-800-662-HELP (4357). Alternatively, you can find this information on their website entitled PA Get Help Now at “apps.ddap.pa.gov/gethelpnow/” that will also help you find local care providers and pill take-back locations based on a zip code.
Other Multimedia Resources
Contributor: Kay Kovitprakornkul, BS, SPT
Next Week: Read Dr. Mackarey’s Health & Exercise Forum – every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquiries related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
ADDICTION: Part 1 of 2.
International Overdose Awareness Day, August 31, 2018
Special Feature “ Health & Exercise Forum” with Geisinger Commonwealth School of Medicine the 3rd Monday of every month!

Sana Chughtai, MD2
Guest Columnist: Sana Chughtai, MD2
Sana Chughtai is a second year medical student at Geisinger Commonwealth School of Medicine from Pittsburgh, PA. She received a Bachelor of Science in Biological Engineering from Purdue University in 2017. Her current interests in medicine include preventative medicine and health education.
“I’m addicted!” It’s a phrase many of us use loosely, whether we’re referring to our favorite snack or our newfound love for a TV show. For some though, the addiction is real. Here in northeastern Pennsylvania the opioid crisis has only gone from bad to worse. Before we can understand the scope of the crisis, we must understand how addiction works. What changes within our bodies and our brains that sparks the start (and continuation of) an addiction?
Whether or not addiction is truly considered a disease is still debated amongst experts in the field, but what is mutually agreed upon is that there are changes in the brain. The first time may have been a choice, but subsequent engagement involves the alteration of normal processes of the brain.
The basal ganglia is often referred to as the brain’s reward circuit. The continuous use of certain drugs, including opiates, over-activates this center, producing what most addicts refer to as a drug high. With repeated exposure of this circuit by the same substance, tolerance is developed. This means that the basal ganglia’s sensitivity is reduced, making it difficult for drug users to feel pleasure from healthy activities that used to bring pleasure before the initiation of drug use. This is one of the factors that leads to dependence, since addicts struggle to feel pleasure from anything other than the drugs they use.
The extended amygdala is involved in handling stressful emotions and is primarily responsible for the feelings of withdrawal. Unlike the basal ganglia, the sensitivity of this area is increased with repeated drug use. This leads to drug-seeking behavior to reduce the unwanted discomfort of withdrawal symptoms.
The prefrontal cortex of the brain is involved in impulse control. Extended drug use can impact the ability of the prefrontal cortex to function properly, leading to impulsive drug-seeking behavior.
 It is also important to understand the role of dopamine in drug addiction. Dopamine is a neurotransmitter, meaning it is a substance released from one neuron (a cell in the nervous system) to act on another. When a person engages in a pleasurable activity, neurons release bursts of dopamine, signaling the brain to associate that particular activity with positive feelings. The purpose of doing so is to form habits and reflexes that increase the frequency of the activity that produces pleasure. Drugs produce larger bursts of dopamine than other, normal routine activities, leading to the formation of the habit.
It is also important to understand the role of dopamine in drug addiction. Dopamine is a neurotransmitter, meaning it is a substance released from one neuron (a cell in the nervous system) to act on another. When a person engages in a pleasurable activity, neurons release bursts of dopamine, signaling the brain to associate that particular activity with positive feelings. The purpose of doing so is to form habits and reflexes that increase the frequency of the activity that produces pleasure. Drugs produce larger bursts of dopamine than other, normal routine activities, leading to the formation of the habit.
There are generations of people that continue to believe that addiction is the result of immorality and weakness and that a strong sense of willpower is all that is needed to overcome it. So many of us are quick to blame addicts for their situations, hindering our ability to truly see it as an affliction that requires legitimate treatment.
Take a lifelong smoker who develops lung cancer for example. The way family, friends, and community members react to this news differs greatly from how many would react if that same individual was acknowledged to suffer from addiction instead. With a cancer diagnosis typically comes feelings of empathy and focus on treatment, while learning of someone’s addiction tends to bring feelings of blame and shame.
But why? People don’t tend to blame the cancer patient for developing his or her cancer, even if their decision to smoke contributed to its development. People do however tend to scrutinize an individual’s addiction and the choice (or series of choices) that led to their dependence.
It’s not always that simple though. Although the term addiction tends to elicit the stereotypical profile of who an addict is, addiction is an affliction that transcends the boundaries of age, sex, skin color, and household income. While many drug addicts’ addictions are a result of illicit drug use, addiction for many others begins with a prescription medication in the absence of any initial illicit activity.
Addiction is a complex issue that requires a complex solution. A simple first step we can all take is to put aside our preconceived notions and cookie-cutter mental images of who addicts are and what addiction entails. We must first change the way we see those who are affected so that we can properly help them in the hopes of improving not only their lives but the lives of family, friends and all those in the communities that have been affected by this plague.
For More Information:
NEXT WEEK: Part 2 of 2, Addiction and Pain Management Alternatives
Read Dr. Mackarey’s Health & Exercise Forum – every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquiries related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
PREVENTION OF HEATSTROKE: For Football, Soccer and Fall Sports
Summer football training camps and practice sessions are in full swing in Northeastern Pennsylvania. A few years ago, the Pennsylvania Interscholastic Athletic Association (PIAA) implemented “Preseason Heat-Acclimatization Guidelines” This policy is slightly updated for starting dates each year (www.piaa.org).
At this time each year, I receive several emails from concerned parents regarding heat stroke in football players and hopefully this column will serve to educate coaches, players and parents about the importance of heatstroke prevention.
Most medical professionals agree that the amount of protective equipment worn by football players makes them more susceptible to heat stroke than athletes in other sports. It is also well-accepted that prevention is the best treatment for heat stroke. They feel that overweight and poorly conditioned players should be monitored closely by weighing in before and after practice. A player who loses more than 3% body weight is at risk for heat stroke. These players should be required to take more breaks, with more fluid intake before, during and after practice. Heat stroke one of the most serious heat-related illnesses. Heat stroke is caused by long term exposure to the sun to the point which a person cannot sweat enough to lower the body temperature. The elderly and infants are most susceptible as are athletes wearing full gear and protective equipment. It can be fatal if not managed properly and immediately. Believe it or not, the exact cause of heatstroke is unclear. Prevention is the best treatment because it can strike suddenly and without warning. It can also occur in non athletes at outdoor concerts, outdoor carnivals, or back yard activities. The American Academy of Pediatrics and The American College of Sports Medicine has the following recommendations:
Gradual Acclimatization to Heat – REFER TO PIAA HEAT-ACCLIMATIZATION Source: www.piaa.org
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
Guest Coauthor: Alexa Rzucidlo, SPT2
Alexa is a second year doctor of physical therapy student at Temple University (2019). She grew up locally in Factoryville, PA. She graduated from Lackawanna Trail High School and Temple University for her undergraduate degree in Kinesiology. Alexa plans to continue her clinical experience at Grand Junction VA in Colorado.
According to the World Health Organization about half of the world’s adult population has had a headache at least once in the past year. For many people, these headaches are infrequent and do not often affect daily life. But what about when your headache occurs frequently or is so severe it prevents you from going about your day to day activities? Some types of headaches are more easily treated and managed than others.
There are two types of headaches: primary and secondary. Primary headaches occur without an underlying disease and include migraines and tension-type headaches. Secondary headaches can be associated with serious disease, requiring emergency care, or can be referred from other structures of the body such as the cervical spine (neck).
Headaches symptoms that may constitute a medical emergency are: vomiting, seizures, fever, muscle pain, night sweat, weight loss, and neurologic symptoms such as blurred vision. If you are experiencing any of these symptoms, if your headache worsens, or your symptoms change it is recommended that you seek medical attention. Any headache that is unusual for you and does not resolve itself in a reasonable time, should be brought to your primary care physician’s attention.
Migraines: Migraines are a primary form of headache that typically lasts from four to seventy two hours, can range from moderate to severe pain, and typically are located on only one side of the head. Often they can be accompanied by an aura, nausea or vomiting, sensitivity to sound, or light sensitivity. Migraines can be aggravated by routine physical activity such as going up stairs. This type of headache is thought to occur in the central nervous system and is related to blood vessels.
Tension-type: Tension-type headaches are the most common primary headache disorder and can last anywhere from thirty minutes to seven days. These headaches can often have a pressing or tightening quality that occurs on both sides of the head. Usually there is no nausea, vomiting, light sensitivity, or aggravation with physical activity. This type of headache is thought to occur in the central nervous system but can have a hereditary component and is usually associated with muscle tender points. Tension – type headaches can be treated with relaxation techniques such as Progressive Muscle Relaxation (PMR), medications, and physical therapy.
The most common secondary headache that is not related to a serious medical condition is a cervicogenic headache (originating from the neck).
Cervicogenic Headache: The length of time a cervicogenic headache can last varies. Usually, the pain is on one side and usually starts in the neck. This type of headache is aggravated or preceded by head postures or movements of the neck. Due to the nerves of the neck and face sharing common connections, pain signals sent from one region can lead to discomfort in the other. Physical therapy can be an effective treatment to help relieve symptoms. For example: posture, exercise, ergonomics, massage, manual techniques, traction, trigger point, and acupressure.
A cervicogenic headache can be caused by an accident or trauma or can stem from neck movement or sustained postures. Sustained postures could mean sitting in front of a computer at work or looking down at your phone. Changing these postures throughout the day could help reduce symptoms. Changing postures could mean bringing your phone closer to you using pillows or another supportive surface when checking social media. If you are someone who works at a desk, it could involve taking breaks or getting a standing desk. However your life requires you to move, there are some simple and effective exercises you can perform throughout the day to help cervicogenic headache symptoms.


Models: Danielle Higgins and Zach Brandt
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
