
Matthew Miraglia – received his Doctor of Physical Therapy degree from Temple University in May of 2019 and an interned at Mackarey Physical Therapy. He grew up in Plains, PA and graduated from Coughlin High School in Wilkes-Barre. Prior to PT school, he received a bachelor of science in kinesiology from Temple University. Matthew plans to graduate with his doctoral degree in May and work in an outpatient physical therapy clinic in the Wilkes-Barre/Scranton Area.
Nearly one million total joint replacement surgeries are performed every year across the United States. A total hip arthroplasty (THA), or hip replacement, is considered to be one of the most successful of all the joint replaced in the body. Moreover, the procedure is considered to be one of the most successful orthopedic interventions of its generation. The procedure has been attempted since the late 19th century, with the modern prosthesis (replacement) seen today being designed in the 1960’s. The modern prosthesis consists of a metal ball and stem, inserted into a plastic cup and secured with acrylic bone cement, technology borrowed from dentists. These mechanical components are referred to as the “low friction arthroplasty”, as it reduces wear and tear of the hip joint. We are currently in the 6th decade of modern THA’s and it is estimated that over 300,000 THA’s are performed each year in the United States alone.
There are many different problems a person might have that may lead a person to undergo a total hip replacement but the most common is severe pain which contributes to loss of mobility and function. Some of the most common reasons for hip pain are: Osteoarthritis – a condition caused by the normal human aging process of joint degeneration; Traumatic Arthritis – when an accident or trauma accelerates the rate of degenerative arthritis; Rheumatoid Arthritis – an autoimmune disorder causing damage to joints throughout the body, including the hip; Hip Fractures – when a hip fracture includes damage to the hip joint; Avascular Necrosis - a condition in which the femoral head does not receive necessary blood supply causing the bone to breakdown; Childhood Hip Diseases – when children are born with certain hip problems, it can lead to early onset of joint damage. Overall, most implants are performed on patients between ages 50-80. However, if you are within this age group and have one of these conditions, this does not necessarily require a hip replacement. In most cases, hip replacements should be considered only after attempting more conservative treatment such as physical therapy, anti-inflammatory drugs, and walking supports or assistive devices in an effort to decrease pain, increase strength of the hip, and normalize daily functions. Hip replacements may be warranted if: conservative treatments have failed; hip pain limits everyday activities such as walking, bending, stair navigation, and sitting; hip pain is unrelenting even with rest; and stiffness that limits ability to move or lift the leg. If you suffer from these problems, you may consider having a conversation with your physician about potential risks and benefits of undergoing a total hip procedure and you may be referred to an orthopedic surgeon for an examination and consultation. The orthopedic surgeon may discuss potential surgical approaches that may be utilized. Anterior (from the front of the hip) and posterior (from the back of the hip) are the two most commonly utilized procedures when performing THA’s. It is important to keep in mind that studies clearly demonstrate that those with significant pain, loss of motion, strength and function become very unhealthy overtime. Due to inactivity they often gain weight, develop high blood pressure and adult onset diabetes. With this in mind, a new hip might be a very wise decision to improve, not only hip function, but overall health.
Posterior Hip Replacement – the posterior approach has been the gold standard in hip replacement since the 1960’s. Its success has been tested over time and is strongly supported in the literature. When using the posterior approach, the surgeon enters from the back of the hip, where the surgeon has a clearer view of the hip joint. In order to achieve this clear view of the hip, the surgeon must cut through various muscles big and small that are key in maintaining the stability of the hip joint and preventing dislocation. While the ease of surgery may be greater with the posterior approach, more soft tissue is compromised which may lead to a longer recovery time, and come with over a month of hip precautions that include no bending, lifting the leg past a certain point (a 90 degree right angle) and crossing legs.
Anterior Hip Replacement – when using an anterior surgical approach, the surgeon is able to work between the muscles in the front of the hip with minimal or no cutting of muscles, leading to a potentially quicker recovery, less pain after surgery, and decreased risk of dislocation, with few or no hip precautions. While the anterior approach is able to avoid disrupting muscles in the front of the hip, the surgeon has a more limited view of the hip joint during surgery and requires navigation through a bundle of nerves that innervate many of the muscles throughout the leg, therefore requiring a skillful and experienced surgeon who consistently performs the anterior approach.
Patients often ask, “Ok, so which one is better?”. The answer to that question though, really has nothing to do with the approach, but has everything to do with the experience of the surgeon. A study from 2016 found that as long as a surgeon is experienced in the technique he/she will perform, there is no significant difference in outcomes between posterior and anterior approaches. Therefore, you should consult with your surgeon to discuss which approach is best for you based on your body type (thin vs heavy), your mental capacity (are willing and able to follow specific approach based precautions) and most importantly, your surgeons preference and experience with a particular approach (how many THA’s and which approach do they perform each year?).
In summary, the purpose of this article is to provide a basic overview of the history of total hip replacements, who may need them and for what conditions, and differences in two of the most common surgical hip replacement approaches, anterior and posterior. In order to know what type of medical management is most appropriate for you, you should consult with an orthopedic and a physical therapist and undergo a comprehensive physical examination that will rule out other sources of pain, and provide you more definitive answers about what is causing you pain at your hip.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week: Read Hip Replacement Part 2
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
Special Feature “ Health & Exercise Forum” with Geisinger Commonwealth School of Medicine the 3rd Monday of every month!
Mary M. Pelkowski, Joseph Hornak, & Cecelia Allison
Mary Pelkowski, MD2 is a student in the Geisinger Commonwealth School of Medicine MD Class of 2022. She grew up in Sayre, PA and graduated from Notre Dame High School. She received her undergraduate degree in biology with a minor in chemistry from Saint John Fisher College in Rochester, NY.
Joseph Hornak, MD received his Doctor of Medicine from GCSOM in May 2019. He grew up in Hazelton, PA. and will train as a resident in Physical Medicine & Rehabilitation at University of California, Davis in Sacramento, CA. Following residency, he plans to pursue fellowship training in pediatric physiatry. Currently, he resides in Allentown, PA, where he is completing his internship year at Lehigh Valley Cedar Crest Hospital.
Cecelia Allison, MD2 medical student at Geisinger Commonwealth School of Medicine. Cecelia grew up in the South Hills of Pittsburgh and graduated from the University of Notre Dame with majors in Neuroscience and Spanish. In her free time, she enjoys practicing yoga and traveling to new places.
Military exoskeleton suits are reality’s version of Marvel’s Iron Man suit. Just as Tony Stark used his suit’s superpowers to fight evil, the military Raytheon XOS 2 exoskeleton suit uses high pressure hydraulics to enhance the wearer’s strength, agility, and endurance. In fact, one soldier in this suit can perform the same amount of work as three army personnel. This has allowed soldiers in the U.S. army to achieve extra-human functions and prevent injuries and strain on their bodies. Industrial exoskeletons use the same design to prevent work related injuries, enhance employee productivity, and extend employees’ time in the workforce. Now, exoskeleton suits have become a groundbreaking medical intervention to help patients who have suffered from spinal cord injuries or strokes.
The preliminary design for exoskeleton suits came from General Electric in the late 1960s. General Electric’s “Hardiman Suit” enhanced the user’s strength, allowing one to lift extremely heavy objects. Researchers soon saw the opportunity for Hardiman technology to restore lost function in people suffering from musculoskeletal problems. In the early 1970s, the Hardiman Suit evolved its first medical use as an exoskeleton, after the work by researchers at the Mihajlo Pupin Institute in Serbia and the University of Wisconsin-Madison in the early 1970s. Since then, exoskeleton suits have focused on teaching or re-teaching users how to walk. The Lokomat (made by the company Hocoma in Switzerland ) was one of the first designs to improve walking abilities of patients who had suffered spinal, cerebral, neurogenic, osseous, and neurogenic injuries. This novel machine is a combination of a treadmill and body weight support, and it allows guided movements and repetition of gait movements to facilitate motoric learning. However, body weight supported treadmill training (BWSTT), like the Lokomat, has not been shown to have any superiority over traditional physical therapy.
Modern, non- BWSTT exoskeleton suits assist patients in achieving over-ground walking in their natural gait pattern (hip extension and full loading of lower limbs) while at the same time promoting active involvement of the patient. The suit, worn over the legs and upper body, contains an intricate network of technology to help its users ambulate. Sensors in the lower limbs capture any postural cue or movement that is initiated by the user. A computer, located in either a backpack or the suit’s torso, will then process this information to activate movements such as sitting, standing, walking, or turning. The exact function depends on the setting that is controlled by a remote worn on the user’s wrist or operated by a licensed therapist. Depending on the extent of the user’s injuries and remaining function, the exoskeleton can be set to completely move the individual’s legs or to assist with the movement, allowing the user to contribute to their own movement however much they are able. While these suits weigh between 50 and 65 pounds, users are still required to use crutches, canes, or walkers to help stabilize their upper bodies and keep the user safe. In the event of a malfunction, the different suits are programmed with failsafe features that lock or slowly collapse the lower limbs.
Currently, the most prominent use for exoskeletons is to help retrain a patient’s gait following an injury or stroke as part of a rehabilitative program with the hope of helping the patient to ultimately regain the ability to walk independently. However, recent FDA approval of the ReWalk exoskeleton for personal use outside of the clinic can provide individuals with a permanent means of maneuvering independently as the exoskeleton can be used at home and in the community. This could impart greater opportunities for freedom and social engagement to the user.Important additional physical benefits of exoskeleton use include increasing physical activity and energy expenditure through the assisted movement of muscles, which may help combat the development of a sedentary lifestyle and obesity. This allows the user to spend less time sitting and more time in an upright position, which may decrease the risks of heart disease and cancer. Furthermore, by helping to support the patient’s weight and movement during rehabilitative exercises, exoskeletons can reduce the physical burden placed on physical therapists in helping patients to execute rehabilitative exercises. Doing so can allow for more effective and efficient utilization of the therapist’s attention to patients. If you are interested in learning more about exoskeletons and their use, rewalk.com and eksobionics.com provide information about their respective suits.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
SPEND TIME OUTDOORS – IT’S HEALTHY!
Part 2 of 2

GET THE HECK OUTSIDE! Research shows that spending time outdoors has many positive effects on your health. While there are many year round activity options, in Northeastern Pennsylvania our short-lived summer is the inspiration to “suck the marrow out of a sunny day!” Summer in NEPA can be enjoyed in many ways such as; walking, running, hiking, biking, horseback riding, boating, kayaking, and swimming. Studies show that even less vigorous activities such as; fishing, picnicking camping, barbequing or reading a good book on the porch are healthier than being indoors.

It is reported that Americans spend 90% of their lives indoors and that number increases with age. Worse yet, for some, venturing outdoors is considered risky behavior with fear of the sun, ticks, wind, mosquitoes and other creatures of God. Well, the truth of the matter is the risk of being one with nature is far less than the ill effects of a life stuck indoors. Please consider the following benefits of spending time outdoors.
Read “Health & Exercise Forum” – Every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
RESEARCH SAYS IT’S HEALTHY!
It is summertime! So, make time to enjoy the great outdoors because research shows that it is good for your health!
Daphne Miller, MD, is a physician, author, hiker and associate clinical professor at The University of California, San Francisco. She is an advocate of the National Park Service’s “Healthy Parks, Healthy People” program. She was featured in NationalParks Magazine for prescribing outdoor activities for the health and well-being of her patients.

Dr. Miller is strong proponent of the spending time in the great outdoors for medicinal purposes. Studies strongly support the fact that exposure to green space has a positive impact on our health and well-being. Consequently, when taking a patient history, she is just a likely to ask a patient how much time they spend in nature, as she is how much they smoke and drink alcohol.

Hundreds of studies support the fact that getting off the couch, away from the television and video games to increase physical activity, is only one of the many reasons people benefit from green space. One study demonstrated that children with attention-deficit hyperactivity disorder (ADHD) functioned with more focus when placed in a natural setting. Other studies found that children demonstrated lower risk for asthma and elderly improved their longevity, when they lived in greener spaces. Most impressive, was a study published in the British medical journal, Lancet, which found that health disparities between wealthy and poor were neutralized when both groups lived in greener spaces.
According to the article in NationalParks, a “nature prescription” written by Dr. Miller might look like this:
Drug: Exercise in Glen Canyon Park
Dose: 45 Minutes of Hiking, Walking, or Running
Directions: Take 3-4 Times per Week (M,W,F,S) at 7 AM or 7 PM
Refill: Unlimited
As many of readers who know me are aware, I am a card carrying member and passionate supporter of the National Park Conservation Association (NPCA). I have not only visited, but camped, explored, and hiked, in many of our National Parks and enjoyed all four seasons in several of these special places. As you may recall from the Ken Burn’s documentary, “The National Parks – America’s Best Idea” these sanctuaries are often described as much for their natural beauty, as they are for the emotion they evoke…spiritual, divine, ethereal, holy, calming, tranquil, mesmerizing, inspirational, illuminating and other countless words of peaceful wisdom. For me, they are this planets version of “heaven!”
WHAT IS YOUR FAVORITE NATIONAL PARK?
People often ask, “What is your favorite National Park?” I tell them, “It is impossible for me to pick just one.” They all have their own special beauty and each exudes a unique feeling. For example, The Grand Canyon in Arizona is an overwhelming beautiful place that must be seen before you leave the planet. For most, it is admired by looking down into a “special version of heaven.” At the same time, Yosemite National Park in California stirs emotion while looking up at the granite rock formed into art by nature with names like Half-Dome and El Capitan. However, more than 500 geysers, including “Old Faithful” and many other thermal features produced over millions of years, have mesmerized visitors in Yellowstone National Park like no other natural feature. And, I will forget how the breathtaking view of Denali Mountain inspires me! (Attached photo by Dr. Greg Cali). So, you can quickly see the dilemma in choosing one favorite over fifty-eight special versions of heaven on earth!
PLENTY OF GREEN SPACE IN NEPA!
Keep in mind, living in NEPA offers plenty of options for healthy green space. You do not have to travel far to get our city or state parks. Nay Aug Park and Lackawanna State Park (attached photo of Dr. Paul Mackarey Jr Kayaking at LSP) are two good LOCAL examples. A short drive will take you to Ricketts Glen State Park for a beautiful hike along the waterfalls. If you don’t mind a little longer drive, The Pennsylvania Grand Canyon will bring you closer to a healthy mind, body and spirit.
Read “Health & Exercise Forum” – Every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
According to the North American Menopause Society (NAMS), 1.5 million American women reach menopause each year. The median age is 52, but some women will reach menopause as early as 40 or as late as 58. Recent research revealed that menopausal women who engaged in three hours of exercise per week for one full year reported improved mental and physical health.
Menopause begins when women’s ovaries are depleted of healthy eggs. Typically, women are born with 1-3 million eggs which are lost over the course of a women’s life through ovulation and other natural means. Under normal conditions, a reproductive hormone called follicle-stimulating hormone, (FSH) stimulates the growth of the eggs during the first half of the menstrual cycle. As a woman approaches menopause, the eggs become more resistant to FSH. Additionally, the ovaries produce significantly less estrogen, a hormone that affects the blood vessels, heart, bone, breasts, uterus, skin and brain. Many of the symptoms associated with menopause are due to the loss of estrogen. These symptoms include: hot flashes, irregular or skipped periods, insomnia, mood swings, fatigue, depression, irritability, racing heart, headaches, joint and muscle pain, decrease sex drive, vaginal dryness, and loss of bladder control. While not all women get these symptoms. Most women experience various degrees of some of these symptoms.
Several studies support the fact that women who engage in regular exercise report less menopausal symptoms than those who are inactive. One particular study in the Journal of Advanced Nursing, found that women who engaged in 3 hours of exercise per week for one full year reported improvement in mental and physical health as compared to the control group. The program consisted of cardiovascular, stretching, strengthening, and relaxation exercises.
In another study published in the Annals of Behavioral Medicine, researchers found that women who walked or performed yoga reported improvements in quality of life with less anxiety and stress related to their menopause symptoms. It is believed that exercise stimulates a release of endorphins in the brain and this is the primary mechanism by which exercise relieves symptoms associated with menopause.
Consult with your family physician before you begin an exercise program, especially if you have health issues. Consider a consultation with an orthopedic or sports physical therapist for professional advice to begin an exercise program best for you. Wear comfortable exercise clothing and sneakers. Exercise to control menopause symptoms does not have to be extreme. A simple increase in daily activity for 15 minutes 2 times per day or 30 minutes 1 time per day is adequate to control your symptoms. This can be simply accomplished by walking, swimming, biking, and playing golf or tennis. For those interested in a more traditional exercise regimen, perform aerobic exercise for 30-45 minutes 4-5 days per week with additional sports and activities for the remainder of the time. For those in poor physical condition, begin slowly. Start walking for 5-10 minutes, 2-3 times per day. Then, add 1-2 minutes each week until you attain a 30-45 minute goal. Keep in mind, weight bearing exercises such as: walking, hiking, and light weight training are important for improving the loss of bone density associated with menopause.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
National Program Comes to NEPA by way of GCSOM
Special Feature “ Health & Exercise Forum” with Geisinger Commonwealth School of Medicine the 3rd Monday of every month!

Cecelia Strauch, MD2 of Factoryville is a member of GCSOM’s MD Class of 2021. She is a member of GCSOM’s Family Medicine Interest Group (FMIG), and served as co-president in 2017-18. She attended Lackawanna Trail High School in Factoryville, and received her undergraduate education at the University of Scranton from which she graduated with majors in biology and philosophy and a minor in Spanish Language.
Geisinger Commonwealth School of Medicine (GCSOM) is teaming up with The Wright Center for Community Health to encourage Scranton residents to take a step toward better health with Walk with a Future Doc, a health program that brings medical students, doctors and patients together to walk every fourth Saturday monthly at 9 a.m. at one of two partner sites: Lackawanna River Heritage Trail at West Olive Street or Backcourt Hoops at 5 West Olive Plaza.
The initiative is led by GCSOM medical student, Cecelia Strauch of Factoryville, a member of the Class of 2021.
Walk with a Doc is a national nonprofit organization whose mission is to encourage healthy physical activity in people of all ages and reverse the consequences of a sedentary lifestyle in order to improve the health and well-being of the country.
“This program has had tremendous participation and success in hundreds of cities around the country,” said Jennifer Joyce, MD, professor of family medicine at GCSOM. “I’m very pleased to bring this exciting and simple program to Scranton because it has shown such improved health results for countless people around the country.”
The walk is open to the community and each walk will feature a short educational talk about a health topic of interest to participants. Participation is free and pre-registration is not required. Walkers will enjoy a refreshing and rejuvenating walk with medical students and healthcare professionals from GCSOM and The Wright Center for Community Health, who will provide support to participants and answer questions during the walk.
“Walk with a Doc is honored to team up with the Geisinger Commonwealth School of Medicine. By incorporating this program into the practice, GCSOM is demonstrating an exceptional level of care and commitment to their community,” said Dr. David Sabgir, founder of Walk with a Doc.
Scranton joins a growing list of communities nationwide that have started local Walk with a Doc (WWAD) programs. WWAD was created by Dr. David Sabgir, a cardiologist with Mount Carmel Health Systems in Columbus, Ohio. He has walked with patients and community members every weekend since 2005.
Learn more about Walk with a Doc at www.walkwithadoc.org.
Benefits of Walking
“There’s no question that increasing exercise, even moderately, reduces the risks of many diseases, including coronary heart disease, breast and colon cancer, and Type 2 diabetes,” said Dr. Jennifer Joyce, MD, professor of family medicine at GCSOM. “Research has even shown that you could gain two hours of life for each hour that you exercise regularly.”
According to the American Heart Association, walking as little as 30 minutes a day can provide the following benefits:
Proper walking technique
Like everything, there is a right way of doing something, even walking. For efficiency and safety, walking with proper stride is important. A fitness stride requires good posture and purposeful movements. Ideally, here's how you'll look when you're walking:
Plan Ahead
Set Realistic Goals
Anything is better than nothing! However, for most healthy adults, the Department of Health and Human Services recommends at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity, or an equivalent combination of moderate and vigorous aerobic activity. The guidelines suggest that you spread out this exercise during the course of a week. Also aim to do strength training exercises of all major muscle groups at least two times a week.
As a general goal, aim for at least 30 minutes of physical activity a day. If you can't set aside that much time, try several short sessions of activity throughout the day. Even small amounts of physical activity are helpful, and accumulated activity throughout the day adds up to provide health benefit.
Remember it's OK to start slowly — especially if you haven't been exercising regularly. You might start with five minutes a day the first week, and then increase your time by five minutes each week until you reach at least 30 minutes.
For even more health benefits, aim for at least 60 minutes of physical activity most days of the week.
Keeping a record of how many steps you take, the distance you walk and how long it takes can help you see where you started from and serve as a source of inspiration. Record these numbers in a walking journal or log them in a spreadsheet or a physical activity app. Another option is to use an electronic device such as a pedometer or fitness tracker to calculate steps and distance
Source: Mayo Clinic
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
High school softball season is over; however, many young women will continue their sport throughout the summer. Unfortunately, female athletes are often forgotten when it comes to injury prevention. It is the purpose of this column to raise the level of awareness regarding prevention of pitching injuries in softball.
Pitching injuries in softball are very similar to the pitching injuries in baseball. Bursitis, rotator cuff injury, impingement syndrome, little league shoulder, little league elbow are all common to the softball player/pitcher. Sherry Werner, Coordinator of the Human Performance Laboratory at the Tulane Institute of Sports Medicine, says that 80 percent of college softball pitchers miss some playing time because of arm pain. Equally startling is that the same problems exist for players in the 12 – 18 age groups. The focus of this article is preventing arm injuries in the softball pitches.
Gerald Warner, a Colorado pitching coach, identified 10 injury-causing softball pitching problems:
CONTRIBUTOR: GARY E. MATTINGLY, PT, PhD, Professor Emeritus, University of Scranton, Dept. of Physical Therapy
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
Get Off Your Butt!
A recent study published in the Journal of the American Medical Association (JAMA) found that the average daily sitting time in the USA has increased by almost an hour over the past decade. This translates to approximately 8 hours of sitting for teenagers and 6 ½ hours for adults in this country. The study found that more than 50% of kids and adults spend more than one hour of LEISURE time per day on a computer. Surprisingly, the greatest increase in sitting time was found among the “oldest” adults. These findings are particularly concerning when one considers the many other studies that have demonstrated the risks of prolonged sitting.
Research has repeatedly correlated the amount of sitting time per day to health problems. In fact, one study found a relationship between the amount of time an individual watches television to a decrease in their average life expectancy. Seriously, watching television and sitting is literally killing us. The Heart and Diabetes Institute of Australia conducted extensive research on sedentary behavior, including a review of almost one million people. They used actuary science, adjusted for smoking, waist circumference, and diet and exercise habits to assess the specific effects that the hours of sitting in a day impacts a person’s life span. They found that sitting too long results in a decrease in muscle contraction of the big leg muscles and because these unused muscles need less fuel, more unused glucose (fuel) is stored in the muscle. High glucose levels result in high blood sugar, which leads to adult onset diabetes and other health issues.
One Hour Sitting (TV) after age 25 = Decrease Life Span by 21.8 Minutes
One Cigarette Smoked after age 25 = Decrease Life Span by 11 Minutes
Six Hours Sitting (TV) over lifetime = Decrease Life Span by 4.8 Years
It is very important to note that exercise alone was NOT the solution. Even people who exercise 30 minutes 3-4 days per week or more, but watch more than six hours of TV, have the same mortality as a non exerciser who does NOT watch TV.
But, if you watch TV AND sit in a chair all day at work in a sedentary occupation, YOUR LONGEVITY IS SHORTENED DRAMATICALLY!
The average adult spends 50 – 70% of their non-sleeping life time sitting. Those with greater sedentary behavior (TV + Sitting Time), have 112% increase risk for adult onset diabetes, 147% increase for cardiovascular disease, 49% increase risk for premature death…even with regular exercise.
Exercise
Exercise is still very important, but you still must sit less and be active in between exercise time.
Limit TV Time
Make a conscious effort to watch less than 2 hours of TV per day. Join the lower risk group.
Get Off Your Butt While Watching TV
When you watch TV, get up and move during every commercial…stand, walk, march in place.
Get Off Your Butt At Office
Every 30 minutes get up and stretch, march in place, or walk for 3-5 minutes. Take the stairs instead of the elevator. Stand up during coffee breaks or when you‘re on the phone. Consider having meetings in which you stand up, use a standing desk or a work station which allows you to walk slowly on a treadmill while you’re working such as a TrekDesk.R (www.trekdesk.com).
In conclusion, don’t kid yourself. Exercise alone will not result in improved longevity if we eat poorly and sit around watching TV the rest of the time. It is about BALANCE…exercise, diet, stress management, and living an active lifestyle with more activity than inactivity. Shut off the TV and get off your butt!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
Paul J. Mackarey, PT, DHSc, OCS is doctor of health science specializing in orthopedic and sports physical therapy. He practices in downtown Scranton and is an associate professor of clinical medicine at GCSOM.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
It happens every spring. A young pitching ace that started strong is now beginning to lose some speed on his fast ball. A third baseman that had no problems last week can’t throw to first base without pain. Shoulder pain in young baseball players occurs every spring just as the first robin, warmer temperatures, and the emerging sprouts of the spring flowers. And, the well-intended father/coach develops severe shoulder pain from hours of throwing balls at batting practice. The cause of the condition was the usual: not properly preparing the arm for the season.
Spring shoulder pain may be prevented with the proper preparation for the season. Throwing a baseball requires the shoulder to be very strong. In the off season, a shoulder can lose much of its essential strength. This loss will result in a deconditioned shoulder at the start of the first spring practice. Practicing with a deconditioned shoulder commonly results in sprain, strain and pain.
To avoid spring shoulder pain it is necessary to maintain shoulder strength. Strengthening exercises need to concentrate on three groups of muscles: the large power muscles of the shoulder, the muscles which stabilize the shoulder and the all important rotator cuff muscles. Strengthening power muscles of the shoulder is fairly easy. Pushups, lat pulldowns, bench presses, and bicep curls will cover all bases. While these exercises are important in maintaining strength and power of the throwing shoulder, they are not as important as the exercises for shoulder stabilizers and rotator cuff muscles.
The shoulder stabilizer muscles connect the arm to the torso. They serve as the foundation of the arm helping to stabilize the arm to the torso. The many stabilizing muscles include the trapezius and the rhomboid muscles.
Exercise for theses muscles include: shrugs, T’s and Y’s. (See Photos A, B, C)
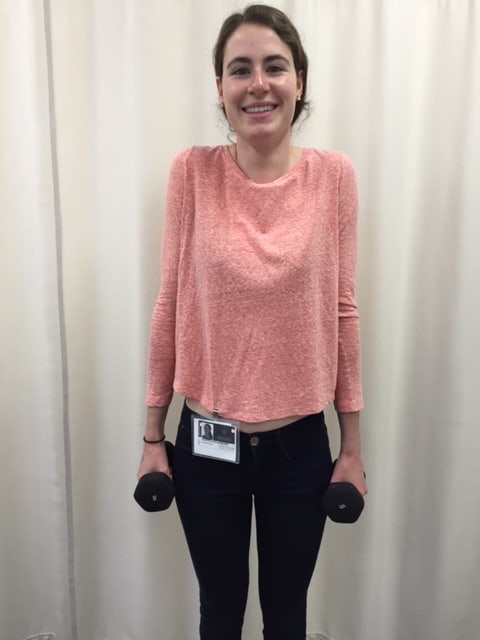


PHOTO A: SHRUGS: Stand with Dumbbell Weight in Hands, Raise Shoulders, Hold 3 Seconds and Repeat 10 times.
PHOTO B: “T’s”: Lying Face Down with Forehead on Towel Roll and With Light Dumbbell Weight in Hands, Raise Arms up in the shape of a “T.”
PHOTO C: “Y’s”: ”: Lying Face Down with Forehead on Towel Roll and With Light Dumbbell Weight in Hands, Raise Arms up in the shape of a “Y.”
The rotator cuff muscles have many functions. They are essential for the stability and proper function of the shoulder joint and in the throwing athlete they serve as brakes during the follow-through phase of a pitch. Exercises for the rotator cuff muscles include internal and external rotations. (See Photos D, E)

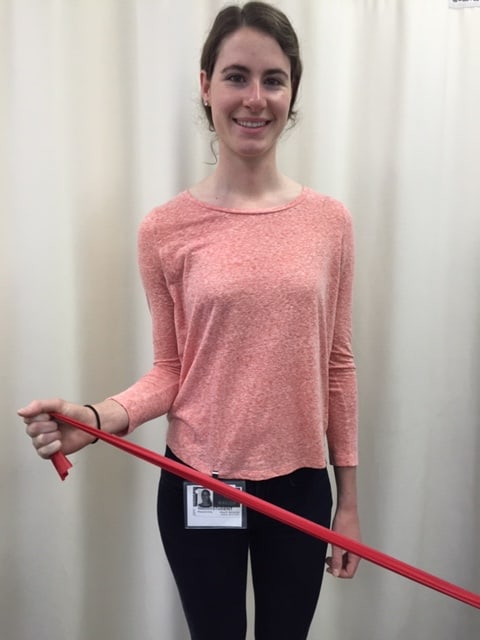
PHOTO D: Shoulder Internal Rotation: Stand with Exercise Band in the Throwing Hand and Elbow at the Side and Bent at 90 degrees, “Turn In - Against the Band.”
PHOTO E: Shoulder External Rotation: Stand with Exercise Band in the Throwing Hand and Elbow at the Side and Bent at 90 degrees, “Turn Out - Against the Band.”
While exercise is essential for conditioning the shoulder in the off-season, a graduated throwing program is also important. In the book The Athlete’s Shoulder, a throwing program is suggested. Training is every other day with a day’s rest in between. A ten minute warmup such as light jogging is suggested before throwing.
Day 1: 45ft – 25 throws - rest - repeat
Day 3: 45ft – 25 throws - rest – repeat – rest – repeat
Day 5: 65ft – 25 throws - rest - repeat
Day 7: 65ft – 25 throws - rest – repeat – rest – repeat
Day 9: 90ft – 25 throws - rest - repeat
Day 11: 90ft – 25 throws - rest – repeat – rest – repeat
Day 13: 120ft – 25 throws - rest - repeat
Day 15: 120ft – 25 throws - rest – repeat – rest – repeat
Day 17: 150ft – 25 throws - rest - repeat
Day 19: 150ft – 25 throws - rest – repeat – rest – repeat
Day 21: 65ft – 25 throws - rest - repeat
Day 23: 65ft – 25 throws - rest – repeat – rest – repeat
With the proper preparation, spring shoulder pain can be avoided in any baseball player.
Contributions: Gary E. Mattingly, PT, PhD is a retired professor at the University of Scranton, Dept of Physical Therapy
Models: Ron Chiavacci,, former professional baseball pitcher; Maggie Reilly, physical therapy student.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
Part 3 of 3
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine.
Guest Author: Timothy D. Welby, MD – board certified pediatrician at Pediatrics of NEPA and associate professor of pediatrics at GCSOM.

For centuries, millions of adults and children died around the world of illnesses that are now preventable with vaccinations. In fact, just a generation ago, most Americans knew a family who lost a child to measles or pertussis (whooping cough). Those of that era also knew someone who had been paralyzed for life by childhood polio. But, thanks to modern medicine and science, this is no longer a common occurrence or fear. For example, in 2000, measles was eliminated in the United States, according to the Centers for Disease Control (CDC). However, since 2000, outbreaks of these preventable diseases have reoccurred. In 2015, almost 200 cases of measles were reported at an amusement park in California. Last year, 18 cases were reported in New York in the Orthodox Jewish Communities and this year the count rises again. What do all these outbreaks have in common? Unvaccinated children!
The purpose of this column over the next few weeks is to discuss the prevention of common childhood diseases using vaccinations and to review potential side effects, both real and imagined.
Despite the overwhelming scientific evidence that childhood immunizations are safe and effective to protect children and adults from serious and potentially fatal diseases, many parents remain skeptical and reluctant to get their children immunized. As with any medication given to millions of patients annually, side effects do occur, however, most are mild and self limiting. Side effects include; redness, swelling or pain at the injection site (usually in the front of the thigh in children and the outer upper arm in adults and children over one). These symptoms are uncomfortable but not dangerous. Mild fever is also common after a vaccine or when multiple vaccines are given together and should be treated with ibuprofen (Motrin, Advil) for children over 6 months old or acetaminophen (Tylenol) for any age child. Fever, especially in a very young child, may not be a side effect to a vaccine but a sign of infection. High fever or lethargy in an infant or child should always prompt a call to the doctor.
Rarely a child can get an infection at the site of a vaccination. It can look similar to a mild reaction but tends to occur a few days after the injection, not immediately following. Also, some children can get a very high fever after vaccination, more likely after the Measles, Mumps, Rubella (MMR) or Measles, Mumps, Rubella, Varicella (MMRV) vaccines which can lead to fever seizures with illness unrelated to the immunization. Measles and chickenpox vaccine can also cause a rash 10 -14 days after immunization, which is harmless but alarming to parents if they are not expecting it.
Measles vaccine may also cause immune thrombocytopenic purpura, a frightening-sounding reaction that occurs when a child’s blood clotting system is affected by the immune system. The condition causes a rash and possible blood clotting problems which can be treated with medication but usually resolves on its own. Rotavirus vaccine, the only oral vaccine routinely given to children, may cause swelling of lymphoid tissue in the intestine called intussusception. It causes a bowel blockage and vomiting and requires urgent medical attention. Fortunately, this reaction is so rare that medical scientists are not sure if it is any more frequent in vaccinated babies as in those unvaccinated. However, what is clear is that prior to routine vaccination against rotavirus, about 60,000 children in the U.S. were hospitalized and 20-60 died each year due to the illness. The most severe reaction to a vaccine is called anaphylaxis. It is a potentially deadly allergic reaction which occur less than one for every million doses administered. However, due to the life-threatening potential of this reaction, immunizations for children should only be administered in a setting fully equipped to handle this emergency.
Some patients with special needs, such as those with illnesses and immune problems, may not be able to receive certain vaccinations. This is not a complete list of reactions to vaccinations. Always ask your physician any questions you have before your child gets their immunizations.
Some parents are hesitant to get their children immunized because they have unfounded fears about vaccine side effects. The biggest recent concerns surround the MMR vaccine and Autism, which arose after a small study linking MMR vaccine and Autism was published in England. The article was discredited and retracted by the journal that printed it. Unfortunately, fear remains despite the fact that there is overwhelming data proving that no connection exists.
Some parents also worry about the effect of multiple vaccines given together might “overwhelm” a young child’s immune system and lead to problems later in life. However, many studies have shown that children with a significant amount of exposures have better immune systems. For example, children who grow up on a farm with a vast number of exposures have better immune systems than their cousins growing up in a city. Ask your family physician or pediatrician … only a phone call away!
In conclusion, the research clearly supports the fact that your child and your community will be far healthier and safer from receiving their vaccinations and the low risk of side-effects and reactions far outweigh the risk of living without vaccination.
For More Information: Center for Disease Control; The American Academy of Pediatrics; the American Academy of Family Physicians
Source: NEPA Vital Signs - The Journal of the Lackawanna County Medical Society
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
