 The Commonwealth Medical College presents: The 1st Annual Keystone Program “Obesity Symposium 2013”
The Commonwealth Medical College presents: The 1st Annual Keystone Program “Obesity Symposium 2013”
In an effort to address the Keystone State’s growing problem with obesity, TCMC with host the 1st Annual Keystone Program – Obesity Symposium 2013 on April 6, 2013.
The World Health Organization has classified obesity as a chronic disease and determined that it is reaching epidemic proportions, not only in the United States, but globally. Moreover, closer to home, the Pennsylvania Department of Health has determined that PA ranks 17th among all states in the country for percentage of obese residents.
The purpose of the symposium is to provide strategies for health professionals and students to prevent childhood and adult obesity recognize risk factors and discuss various treatment options such as behavioral, pharmacological, and surgical.
“Health & Exercise Forum” will dedicate the next two weeks to a topic related to this local, national and international epidemic by Ryan Sugarman, 4th year medical student at TCMC.
Part 1 of 2 on Bariatric Surgery
Guest Columnist: Ryan Sugarman, 4th Year Medical Student TCMC
Ryan Sugarman is a 4th year medical student and member of the charter class of The Commonwealth Medical College (TCMC). He was raised in Long Island, NY and earned a Bachelor of Science in Chemistry at Tufts University. He has a special interest in preventive care and has researched diabetic foot care and ways to improve pneumonia vaccination in the Scranton area. Recently he investigated the average one year weight loss of three bariatric procedures performed at Wilkes-Barre General Hospital in Wilkes-Barre, PA. He is currently applying for Internal Medicine residency and plans to complete a fellowship in gastroenterology, nephrology or hematology/oncology afterward.
Nearly one of three Pennsylvanians is obese, quantified as a Body Mass Index (BMI) > 30. This places them at risk for diabetes, hypertension (HTN) or high blood pressure, obstructive sleep apnea (OSA), and many other diseases. These illnesses may be insidious, festering unnoticed until they cause a stroke or heart failure. While diet and exercise are encouraged, it is often not enough to be effective. In more severe cases, surgical measures should be considered based on specific criteria to be discussed later in this column.
Bariatric surgery is an operation designed to help a patient lose weight. There are different types of bariatric surgery which restrict nutrient intake (restrictive) and/or restrict absorption of food (malabsorptive). Three examples that are commonly done at Wilkes-Barre General Hospital are discussed in more detail below.
1) Gastric Band
This is a type of surgery in which an adjustable band is placed around the stomach. This band can be thought of as a belt which can be tightened or loosened as needed in the outpatient setting. The band restricts the rate that the stomach can fill.
2) Gastric Sleeve
This operation removes a large portion of the stomach, leaving behind only a small “sleeve” which is roughly the size of a banana. Not only is this surgery restrictive, but it also has a hormonal mechanism promoting weight loss. The stomach secretes a hormone, ghrelin, which stimulates hunger. By removing most of the stomach, ghrelin secretion is decreased so there is less sensation of hunger.
3) Roux-en-Y Gastric Bypass
This complicated surgery rearranges the gastrointestinal (GI) tract so there is less time for the absorption of nutrients to occur. The procedure also decreases stomach size to a gastric pouch which reduces its storage capacity.
The results vary as by case, but research has shown a dramatic benefit in long term survival of morbidly obese patients who undergo bariatric surgery. Obesity related diseases such as HTN and diabetes may resolve.
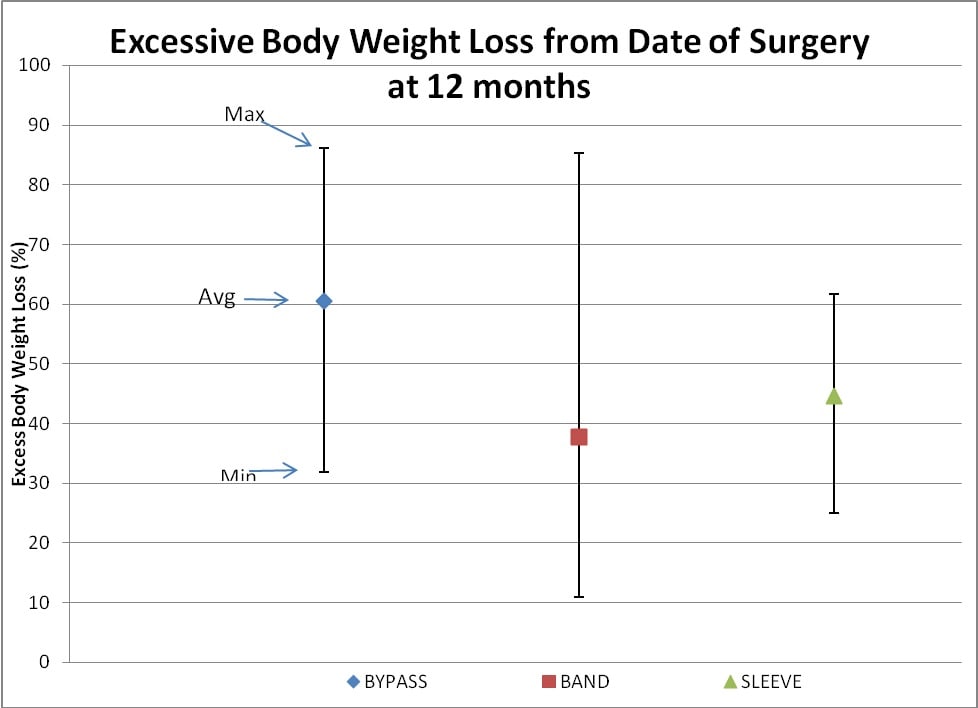
A recent research project of Wilkes-Barre General Hospital bariatric surgery patients compared their one year excess body weight loss (EBWL) results. The gastric band, gastric sleeve, and gastric bypass patients had EBWL of 38%, 45% and 60% respectively. The results are demonstrated below.
Adam Pascoe, coauthor of the project and a fourth year medical student at TCMC, said “Being a Tunkhannock native I wanted to give back to the area by educating people that these (procedures) should not be viewed as cosmetic surgeries, but rather life extending surgeries.”
The National Institute of Health (NIH) recommends bariatric surgery for those who are extremely obese as defined as a Body Mass Index (BMI) > 40) or those who are morbidly obese as a BMI > 35 with coexisting illness such HTN. You may calculate your own BMI by multiplying your weight in pounds by 703 and dividing by your height in inches squared. For example, a person weighing 200 pounds and is 5 feet 2 inches tall has a BMI of 36.5 and is well over the standard for obesity and morbid obesity according to BMI charts.
Body Mass Index (BMI) Chart
BMI 18.5 under weight
BMI 18.5 – 24.9 normal
BMI 25 – 29.9 overweight
BMI > 30 obese
BMI > 35 morbidly obese
Anyone interested in bariatric surgery are required to attempt a serious diet and have their medical history reviewed before they qualify. A psychiatric evaluation and upper endoscopy to visualize their digestive tract may also be required.
Dr. Clark Gerhart and Dr. Gary Neale, general surgeons who operate at Wilkes-Barre General Hospital, offer free seminars about the surgery to the public twice a month in Wilkes-Barre and as of 2013 there will also be a monthly meeting at Scranton Regional Hospital. Dr. Neale said “These (meetings) allow patients to better understand the surgery they are considering and gives an opportunity to ask questions without the time and expense of making an appointment. “ He added “With the program now entering its third year we are seeing friends and family of previous patients, who have witnessed the benefits and success that the individual has obtained through weight loss surgery.” Information about these seminars can be found at http://www.wilkesbarregeneral.
Next week we will discuss risks, benefits and outcomes of bariatric surgery.
NOTE: Images in article were reproduced with permission of Dr. Gianfranco Silecchia MD PHD FASMBS, Associate Professor of Surgery at Padiglione Universitario, Rome, Italy.
Read Dr. Mackarey’s Health & Exercise Forum in the Scranton Times-Tribune – every Monday…Next Monday Read “Bariatric Surgery - Part II
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
 The Commonwealth Medical College presents: The 1st Annual Keystone Program “Obesity Symposium 2013”
The Commonwealth Medical College presents: The 1st Annual Keystone Program “Obesity Symposium 2013”
In an effort to address the Keystone State’s growing problem with obesity, TCMC with host the 1st Annual Keystone Program – Obesity Symposium 2013 on April 6, 2013.
The World Health Organization has classified obesity as a chronic disease and determined that it is reaching epidemic proportions, not only in the United States, but globally. Moreover, closer to home, the Pennsylvania Department of Health has determined that PA ranks 17th among all states in the country for percentage of obese residents.
The purpose of the symposium is to provide strategies for health professionals and students to prevent childhood and adult obesity recognize risk factors and discuss various treatment options such as behavioral, pharmacological, and surgical.
“Health & Exercise Forum” will dedicate the next three weeks presenting columns on topics related to this local, national and international epidemic.
People have theorized for many years that obesity must be genetic. Scientific research has validated this theory and more importantly, a recent study has shown that while there is an obesity gene that may predispose one to obesity, one can control the outcome with exercise. The fat mass and obesity gene (FTO) is linked to a high body mass index according to a new study in the Archives of Internal Medicine. More importantly, this study found that exercise can offset a genetic predisposition for obesity. Aerobic exercise 30-45 minutes 3-5 times per week coupled with mild weight training and other physical activities can overcome the FTO. With new knowledge, it becomes apparent that it is critical to promote a healthy lifestyle with exercise and physical activity at an early age to prevent childhood obesity.
Childhood obesity is defined as an excessive accumulation of body fat, as determined by skinfold measurements, when the total body weight is more than 25 percent fat in boys and 32 percent in girls. While some define it as a weight/height in excess of 120 percent of the ideal, skinfold measurements have been found to be much more accurate.
Childhood obesity has reached epidemic proportions in the United States. Moreover, childhood obesity is on the increase as found in a 54 percent increase in body fat measurements among 6-11 year olds since the 1960’s. The American Medical Association and American Physical Therapy Association have taken active rolls through their memberships to educate, advise and treat children with weight problems:
Obesity increases with age and its prevalence among obese children will continue to be obese with age. Childhood obesity is the leading cause or is associated with: hypertension, Type II diabetes mellitus, coronary heart disease, lower extremity joint stress and pain, lower self-esteem and other psychological problems.
As with adult obesity, childhood obesity is most often caused by multiple problems including: nutritional, psychological, familial, and physiological.
Weight loss is not the primary role of a good childhood obesity program. The goal is to limit or stop weight gain so the child will eventually grow into their body weight over a period of many months or years. One study suggests that it requires 1 ½ years of body weight maintenance for every 20 percent excess in ideal body weight for a child to ultimately attain ideal body weight.
Increasing physical activity or engaging in a formal exercise program is essential to burn fat, increase caloric expenditure to lose and/or maintain weight. However, studies show that exercise alone is not nearly as effective as when it is combined with proper nutrition/diet and behavior modification. Physical activity is also critical for the health of the child. Blood pressure and lipid profiles improved in children/adolescents who engaged in 50 minutes of aerobic exercise, 3 times per week, even when weight loss was only minimal. In view of this, I recommend 45-60 minutes of exercise and physical activity a minimum of 5 days per week and prefer 7.
Use technology to promote fitness with physically active video games such as the Dance, Dance Revolution (DDR) or Wii Fitness to excite your kids into healthy activity. A recent study at the Mayo Clinic has found that children expended significant energy when they play video games that require activity, such as the “NintendoR Wii.” The study found that kids expended three times more energy as compared to traditional video games played while sitting or when compared to watching TV while walking on a treadmill. There may be hope for our kids!
Also, some exercise and fitness clubs specialize in programs exclusively for children such as Fitwize 4 Kids. It is a kid’s health club that offers an assisted 45 minute program featuring cardio, strengthening, flexibility, agility and nutritional counseling for ages 6 ½ to 15. www.Fitwize4Kids.com
Extreme dieting and fasting is not appropriate for children. It is emotionally stressful and physically harmful to the growth and development of a child/adolescent. A balanced diet with moderate caloric and portion restrictions coupled with exercise and counseling is the proper combination.
Behavioral strategies are found to be very successful in children/adolescence. Self-monitoring and keeping a record in a journal of food intake, activity and exercise are helpful. Also, rewards and incentives can be effective. Parent/child counseling programs are most effective.
In conclusion, childhood obesity is a serious epidemic. It is physically and emotionally stressful for the child/adolescent and family. This problem requires a comprehensive team approach including: physician, educator, dietitian, psychologist, and exercise specialist. Lastly, to be successful, it must be a lifetime lifestyle change 7 days a week with regard to diet and exercise, not a 3 to 6 month fad. It must be a long-term program with long-term goals.
Visit: www.NintendoWii.com, www.dance-revolution.com, www.fitwize4kids.com
Sources: Archives of Physical Medicine, 2008, Vol 168, 1791 – 1797
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune. Next Week: Bariatric Surgery for Obesity Part I of II.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 2 of 2
Spring has sprung! Dust off your bikes and discover the beauty and challenge of biking in NEPA. Whether you are a rural or urban dweller, the Countryside Conservancy Trails at Lackawanna State Park or the Lackawanna Heritage Valley Authority trails can meet your needs.
By my view, Tour de Scranton is the official “kick off to the local biking season.” This year, on Sunday, April 28th, the 10th annual Tour de Scranton will offer a selection of several routes and distances for the novice and experienced rider at its non-competitive bike ride for riders of every age and skill level. This event supports “The Erin Jessica Moreken Drug & Alcohol Treatment Fund” which provides charitable gifts to qualified local organizations or individuals struggling with the disease of addiction. For more information visit: www.tourdescranton.com.
Whether you are a recreational bicyclist or competitive cyclist it is critical that you and your bike fit well together. A proper fit maximizes comfort and minimizes injury. Last week we discussed how to position handlebars, pedals, seat, at proper angles for the shoulders, trunk, hips and knees. This week, I would like to discuss the benefits of cardiovascular exercise and common problems that develop from biking on an improperly fitted bike.
Biking, like all aerobic exercise, provides all of the following benefits without the added stress of joint compression, and wear and tear associated with many other full weight bearing exercises such as running:
Prevention is the best management of musculoskeletal problems associated with biking. First, as previously discussed in Part I, prevent many of the above problems through proper fitting. Furthermore, it is important that your equipment is in good working order such as tires, chain, brakes and pedals. Next, be sure to maintain a fairly good fitness level in order to bike safely. If you are a beginner, start slowly. Warm up and slowly bike for 10 to 15 minutes and build up over time. Practice the coordination of stopping, starting, shifting and braking. Work on good strength and flexibility of the hamstrings, quadriceps, calfs and gluteal muscles. All of these muscles are necessary to generate pedal force. Balance is also important to safety and can be practiced on and off the bike. Be aware that adaptive equipment can modify your bike for added comfort and safety such as soft handlebar tape, seat post and front fork shock absorbers, cut-out and gel pad saddle seats, and wider tires. Remember, WEAR A HELMET!
Be careful not to progress too quickly because inactivity to over activity in a short period of time can create problems. Overuse injuries such as tendonitis, can be avoided by cross training. Bike every other day and walk, run or swim on off days. Consider sports such as tennis, golf, racquetball on off days. Make sure to take time off to recover after a long ride. Use ice and massage to sore muscles and joints after riding.
Remember, cycling should be fun! Pain from improper fitted and poorly maintained equipment is preventable. Excessive workouts and training rides should be kept to a minimum.
SOURCES: American Physical Therapy Association
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 1 of 2
Spring has sprung! Dust off your bikes and discover the beauty and challenge of biking in NEPA. Whether you are an rural or urban dweller, the Countryside Conservancy Trails at Lackawanna State Park or the Lackawanna Heritage Valley Authority Trails can meet your needs.
By my view, Tour de Scranton is the official “kick off to the local biking season.” This year, on Sunday, April 28th, the 10th annual Tour de Scranton will offer a selection of several routes and distances for the novice and experienced rider at its non-competitive bike ride for riders of every age and skill level. This event supports “The Erin Jessica Moreken Drug & Alcohol Treatment Fund” which provides charitable gifts to qualified local organizations or individuals struggling with the disease of addiction. For more information visit: www.tourdescranton.com.
Bicycle riding is a great way to get cardiovascular exercise. It is easy, can be done indoors on a stationary bike or outdoors weather permitting. It is kind to your hip, knee and ankle joints. It can be inexpensive and enjoyed by the entire family. However, if not done properly, it can lead to problems. A poorly fitted bike can lead to hip, knee and ankle pain, tendonitis, or back and neck pain. Also, an improper fitting seat can lead to pain and numbness in the peritoneum or saddle and lead to prostrate inflammation and erectile dysfunction.
The good news is that with a little effort a properly fitted bike can offer many safe miles of great exercise and health problems can be avoided. The Canadian Physiotherapy Association, Dr. Gerald Gilbert and Dr. Ira Cohen, urologists and cycling enthusiasts and Eugene Geeza, physical therapist and cyclist have assisted me in compiling the following recommendations:
Frame size is one of the most important steps to insure a good fit. To be sure that the frame of the bike is right for you, stand over the top cross-bar between the seat and the handlebars. Road bikes should allow 1 inch between the bar and your buttocks while a mountain bike requires 2 to 6 inches of space depending on the terrain and slope of the trail that may require you to get your feet to the ground quickly.
The saddle or seat should be as level as possible. If the seat tilts forward, then you will feel as if you are falling off the seat and your arms and back may take too much weight and stress. If your seat tilts backwards, then you will strain your lower back and too much stress will be placed on your buttocks and saddle area leading to discomfort. Proper saddle height should allow your leg to be just short of full extension, (a 10 to 20 degree angle) without locking the knee, at the bottom of the pedal stroke. If you are shifting your weight with each revolution, then your seat is too high.
Handlebar position has a direct effect on the comfort of your neck, middle and lower back while biking. If the bars are too low or too forward, it will force the rider to stretch and lean over and forward too far. This will stress the spine. If the bars are too high and back, it will force the rider to sit back too far and place more weight on the buttocks and saddle. As a rule, a taller rider is better with a bar that is lower than the saddle height and shorter riders are even or slightly above.
Misalignment of the feet while riding and pedaling repeatedly over many miles can create undue discomfort. In most cases, your feet should point straight ahead. However, due to unique differences in pelvis, hip, and lower leg alignment, a slightly toed out foot (10 to 20 degrees) may be necessary to prevent twisting stress in the legs as you pedal.
EQUIPMENT: Helmets are a must! Also, keep your bike in good condition. Road bikes should have mirrors, reflectors and obey traffic rules. Use hand signals. Dress for weather and visibility. Have a first aide and tire patch kit, pump and tools. Seat comfort can be improved with gel cushion or split seat.
BE ALERT: for traffic, parked cars, pedestrians loose gravel and cracks in the road.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune Next Monday: Cycling Part II of II.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
 Part 2 of 2
Part 2 of 2
Guest Author: Nicholas J. Russo, The Commonwealth Medical College
Guest Author: Nicholas J. Russo, is a recent honors graduate of the Master of Biomedical Sciences Program at The Commonwealth Medical College (TCMC) where he participated in several research and community service projects. He received his Bachelor of Science Degree in Technological Systems Management Engineering and Biology from Stony Brook University in New York and plans to continue his education in medicine.
Trust is a necessary component to a happy, healthy and well-balanced life. However, it is not without its risks. But, when the trust is warranted, the risk is worth the benefit. New research shows that patients, who trust their physicians, have better outcomes…the doctor-patient relationship matters!
5 Ways Patients Feel Trust:
The general consensus for patients with whom I have spoken is that they want to be heard. They want to know that their doctor truly cares about them and is going to go that “extra mile” for them when it counts. An article published in the Strategic Medicine Journal, reinforces trust as being a major factor for improving healthcare outcomes.
Physicians who seem to be the most successful in establishing trust demonstrate that “they care” one gentleman stated. It was more important for this patient feel special…not “feel like just another number.” While you may wait 45 – 60 minutes to see the physician, once seen, if needed, the same 45-60 minutes is spend directly with you.
Physicians should treat the patient as if they are intellectually capable of understanding the problem, when appropriate, and provides resources, websites, reading and material for further discussion on the next visit. It is also important that the physician and his staff respond appropriately to you questions and concerns.
An anonymous patient revealed that he appreciates that his new physician tries to bring a personal touch to the conversation as it makes him feel more connected and more eager to trust. This same patient said that since switching to his new physician, he has noticed that his blood pressure and diabetes have been well controlled and he feels incredible.
While a physician does not have to be your best friend, they should make time to get to know you as more than the “overweight diabetic with high blood pressure.” For example, it might be important to know that you spend every weekend in the woods hiking and camping which may make you more vulnerable to deer ticks and . It might also be valuable to know that you have a high pain threshold and rarely overreact.
While nurse practitioners and physician assistants are well-educated and an essential part of the delivery of quality healthcare, it is important to know that your care is being overseen by your physician. This can be accomplished by a quick visit in the treatment room or a follow-up phone call. Either way, it is important to see your physician at least 50% of the time you visit the office.
Does someone from the physician’s office return you phone calls promptly? Does the office contact you with information regarding the outcome of your tests (MRI, X-ray or blood tests, etc)?
In conclusion, it is important to have a good “doctor-patient relationship” to improve compliance, satisfaction and outcomes. Most patients believe that the quality of time is really the determining factor for whether or not they trust their doctor. “I don’t expect the doctor to know everything there is to know about me but I do expect that for the time they are with me I feel as though I am heard,” an anonymous patient said.
As a student hoping to care for you and your family as a physician, one day, I whole heartedly believe that quality healthcare begins with a foundation of trust. What I have learned at TCMC so far is that trust is an important beginning of a great doctor-patient relationship that ultimately ends with the delivery of quality healthcare.
I encourage all patients to work with your physician to establish a relationship built on trust… to the degree that you would sign a blank check over to your physician, like Amos and believe that by trusting them with your life you are undoubting improving your health as well.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum" in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in Scranton, PA and is an associate clinical professor of medicine at The Commonwealth Medical College.
Guest Author: Nicholas J. Russo, The Commonwealth Medical College MBS Class of 2012
The New Doctor-Patient Relationship
Part I of II
Guest Author: Nicholas J. Russo, is a recent honors graduate of the Masters of Biomedical Sciences Program at The Commonwealth Medical College (TCMC) where he participated in several research and community service projects. He received his Bachelor of Science Degree in Technological Systems Management Engineering and Biology from Stony Brook University in New York and plans to continue his education in medicine.
In NEPA our communities are grounded in trust. On a regular basis, a senior citizen comes to my office for a consultation and the first question they ask me is, “Who is your father, Paul?” This question is followed by, “Was Al your uncle?” “Are you related to Mike?”
While I was not sure of the importance of these questions early in my career, I have come to realize that patients were just trying to make a connection with me. They wanted to know if they could “trust” me. Nick Russo, recent graduate from TCMC’s Masterof Biomedical Sciences Program, presents new research which supports their instincts; patients who trust their healthcare provider have better outcomes…the doctor-patient relationship matters!
Amos was an Amish patient treated for pneumonia with penicillin injections by Dr. Henry. On the last day of his regimen, Henry told Amos that he did not have a bill prepared and asked him to return another day. Amos replied by writing a blank check. Henry refused the blank check as he explained that he could write in any amount he wishes. Amos replied without hesitation, “I trusted you with my life. I do not see why I cannot trust you with my money.”
This quote from the book “Patients Are a Virtue,” by Henry S. Wentz demonstrates that trust is an essential component of the doctor-patient relationship. The sanctity of the Doctor-Patient relationship is the very essence of quality healthcare and is the basis for patient satisfaction and positive outcomes. Recent studies show that patients feel strongly that trust should be the number one factor when it comes to choosing the “Right” physician for you.
A recent study published in the Internal Journal of Medical Education, has demonstrated that better patient outcomes and compliance to treatment increase when doctors are trusted and more proactive in involving their patients with their own healthcare. Patients agreed that they trusted their doctors more when extra time was spent explaining the procedure and treatment, the author explained. These patients were more likely to get regular check-ups, medical tests and take their medications properly. They are also more likely to follow a healthy lifestyle including diet and exercise and control diseases such as blood pressure and diabetes.
Trusting your physician plays a much larger role than one would imagine when making medically informed decisions. Dr. Janet Townsend, founding Chair of the Department of Family, Community and Rural Health at The Commonwealth Medical College (TCMC) believes that establishing a foundation of trust with a patient and their loved ones is the basis for delivering quality healthcare. She expressed that, “People need to trust you as a doctor and know that you are truly here for them.” Dr. Townsend’s experiences have taught her that there is no simple equation for establishing trust but it is a powerful tool for improving patient outcomes.
Dr. Mark White, an educator and community health researcher at TCMC, takes great pride in his Physician and Society course for first year medical students. Dr. White believes that trust is an intricate aspect of the doctor-patient relationship; it is the root of passionate patient centered medicine, something he emphasizes in his curriculum.
“Doctor-Patient Relationships Improving”, an MSNBC article, presents a compelling argument that the original “authoritative attitude” of the doctor with their patients has rapidly become a thing of the past. More and more patients are taking responsibility for their health education and this article suggests that trust is the key underlying factor that allows this open communication which serves to better patient treatment.
Today’s doctor-patient relationship is one where both parties are now more equal than ever and this allows both parties to be rewarded for establishing lasting relationships built on trust.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum in the Scranton Times-Tribune-Part II of II: “The New Doctor-Patient Relationship.”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in Scranton, PA and is an associate clinical professor of medicine at The Commonwealth Medical College.
Last week in Part I on Depression I discussed the importance of laughter for the prevention of depression. In this column, I will discuss one of the most understated benefits of exercise – mental health! Specifically, aerobic exercise (exercise that increases your heart rate for 30 minutes or more) such as walking, biking, running, swimming, hiking, elliptical & stepper machines to name a few, is the secret to “runner’s high.” This exercise euphoria is not limited to runners alone, but all who engage in aerobic exercise are more likely to experience high energy, positive attitude, and mental wellness.
Physical activity, specifically aerobic exercise, is a scientifically proven useful tool for preventing and easing depression symptoms. Studies in the British Journal of Medicine and the Journal of Exercise and Sports Science found that depression scores were significantly reduced in groups that engaged in aerobic running, jogging or walking programs, 30-45 minutes 3-5 days per week for 10-12 weeks, when compared to a control group and a psychotherapy counseling group.
Depression is the most common mental disorder and is twice as common among women as in men. Symptoms include: fatigue, sleeplessness, decreased appetite, decreased sexual interest, weight change, and constipation. Many of these symptoms are likely to bring an individual to their family physician. Unfortunately, depression is on the increase in the United States. According to the National Ambulatory Medical Care Survey, in the 1990’s, 7 million visits to a primary care physician were for the treatment of depression. 10 years later the number doubled.
According to research reported in The Physical and Sportsmedicine, exercise reduces depression in two ways, psychologically (mentally) and physiological (physically).
Psychological or Mental Benefits of Exercise on Depression:
Physiological or Physical Benefits of Exercise on Depression:
Read Dr. Mackarey’s Health & Exercise Forum in the Scranton Times-Tribune – every Monday
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
The decorations are long gone. Family and friends are back to their routines. The bills from the holidays have arrived and winter has hit hard with too many short, cold, dark and dreary days. It only takes a few other problems like stress at work and health issues to put you over the edge…
Depression is the most common mental disorder and is twice as common among women as in men. It impacts life in many ways; family, friends, work, play and general health. Symptoms include: fatigue, sleeplessness, decreased appetite, decreased sexual interest, weight change, and constipation. Many of these symptoms are likely to bring an individual to their family physician. Unfortunately, depression is on the increase in the United States. According to the National Ambulatory Medical Care Survey, in the 1990’s, 7 million visits to a primary care physician were for the treatment of depression. 10 years later the number doubled.
Recent research is very encouraging and supports the use of laughter and exercise to prevent and treat depression as a powerful adjunct to therapy and medication. While it is important to state that depression is no laughing matter, many mental health professionals support it as a method to confront an unpleasant situation and gain some level of control over it. One study showed that in elderly people who used humor on a regular basis, reported improved satisfaction in life as compared to their less humorous contemporaries.
(based on recent studies)
Sources: LifeScript.com. If you or someone you know is in danger from depression contact the American Foundation For Suicide Prevention at 1-888-333-2377.
Read Dr. Mackarey’s Health & Exercise Forum in the Scranton Times-Tribune – every Monday. Next Week, Part II of II - Exercise to Prevent Depression.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
Mim Joseph, a librarian retired from the North Pocono School District, is someone whom I have held in high regard for many years. She has been retired from her career for many years but has not retired from life…she is open-minded, intellectually curious and reads incessantly. She remains active despite some recent health issues and makes a significant effort to “stay off her butt!” She recently read an article in the New York Times about the perils of sitting too much and thought it was a good topic for my readers…I agree. Thank you, Mim.
Recent research has correlated the amount of time an individual watches television to a decrease in their average life expectancy. Seriously, watching television and sitting is literally killing us. The Heart and Diabetes Institute of Australia conducted extensive research on sedentary behavior, including a review of almost one million people. They used actuary science, adjusted for smoking, waist circumference, and diet and exercise habits to assess the specific effects that the hours of sitting in a day impacts a person’s life span. They found that sitting too long results in a decrease in muscle contraction of the big leg muscles and because these unused muscles need less fuel, more unused glucose (fuel) is stored in the muscle. High glucose levels result in high blood sugar, which leads to adult onset diabetes and other health issues.
It is very important to note that exercise alone was NOT the solution. Even people who exercise 30 minutes 3-4 days per week or more, but watch more than six hours of TV, have the same mortality as a non exerciser who does NOT watch TV.
But, if you watch TV AND sit in a chair all day at work in a sedentary occupation, YOUR LONGEVITY IS SHORTENED DRAMATICALLY!
The average adult spends 50 – 70% of their non-sleeping life time sitting. Those with greater sedentary behavior (TV + Sitting Time), have 112% increase risk for adult onset diabetes, 147% increase for cardiovascular disease, 49% increase risk for premature death…even with regular exercise.
Exercise
Exercise is still very important, but you still must sit less and be active in between exercise time.
Limit TV Time
Make a conscious effort to watch less than 2 hours of TV per day. Join the lower risk group.
Get Off Your Butt While Watching TV
When you watch TV, get up and move during every commercial…stand, walk, march in place.
Get Off Your Butt At Office
Every 30 minutes get up and stretch, march in place, or walk for 3-5 minutes. Take the stairs instead of the elevator. Stand up during coffee breaks or when you‘re on the phone. Consider having meetings in which you stand up, use a standing desk or a work station which allows you to walk slowly on a treadmill while you’re working such as a TrekDesk.R (www.trekdesk.com).
In conclusion, don’t kid yourself. Exercise alone will not result in improved longevity if we eat poorly and sit around watching TV the rest of the time. It is about BALANCE…exercise, diet, stress management, and living an active lifestyle with more activity than inactivity. Shut off the TV and get off your butt!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
Paul J. Mackarey, PT, DHSc, OCS is doctor of health science specializing in orthopedic and sports physical therapy. He practices in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
In 2013, "Health & Exercise Forum" will begin a new and exciting journey. Beginning the first two Mondays of the new year, students from The Commonwealth Medical College author columns on a regular basis throughout the year. TCMC students have worked long and hard in 2012 researching, discussing and drafting columns in between their rigorous medical studies. It will be the purpose of this collaboration, not only to provide new and exciting information on healthcare to the public, but also to introduce you to the many of the students at TCMC...Your Medical College! Working with the students over the past year has been my pleasure and privilege. They are bright, eager, enthusiastic, and altruistic. While many students (70%) are residents of Pennsylvania, others, as you will see, come from many interesting places and bring with them a wealth of life experiences to make our college and community more interesting. They are more than full-time medical students, as they take time from their studies to contribute to our community by participating in community service. Guest Columnist: Steven J. Scheinman, MD, President and Dean, The Commonwealth Medical College
Happy New Year!
The coming of a new year is a time of hope for fresh beginnings and, for many of us, resolutions to take better care of ourselves. At The Commonwealth Medical College, 2013 promises to be a very significant new year indeed.
On “Match Day” in March, our charter class, who are now seniors, will learn where they will be doing their residency training. We already know that they are doing very well in getting invited for interviews, and are getting honors grades in the elective rotations they are doing at other medical schools. Our two seniors with military obligations have already had good news in the “Military Match” which takes place in December. Trevor Echelmeier, from Ardmore, matched at Madigan Army Medical Center, and Scott Dalane, from Philadelphia, matched at the Walter Reed National Military Medical Center. These were the first choices for both Trevor and Scott.
On May 11, the vision of the founders of TCMC will be realized with the graduation of our first MD class. Our accrediting agency, pleased with our success, has approved expansion of our MD class to 100 members. The class of 2017, who are being selected now, will enter TCMC in August.
We are very proud of our students, whose passing rate on board exams has exceeded the national average for both of our first two years. Seventy percent of them are from Pennsylvania, more than at any other medical school in the state. Students in all four classes engage in community service projects and research projects in community health throughout the region. Many of them will be contributing to this column throughout the coming year. Lani Hossain is president of the TCMC Journalism Club and the recipient of the first annual Healthcare Journalism Award. Lani will be the first of our medical student journalists who will publish in “Health & Exercise Forum” in The Times-Tribune this year.
We have reached a point where we now have objective corroboration that our innovative curriculum is serving our students so well. This is a remarkable achievement in which the founders of the school, and its faculty and staff, can take justifiable pride. But producing new doctors for northeastern Pennsylvania is only one part of our mission. Our aim is no less than to transform medical care in the region. That may seem a tall order for an independent medical school without its own hospital or practice plan. We will do this through partnerships.
We have begun by convening leaders from hospitals, healthcare systems, physicians, residency programs, and others from across our 16-county region on a collaborative plan to improve healthcare quality. While we are fortunate to have wonderful hospitals in this region, every healthcare institution strives to deliver care that is excellent and error free. By convening this set of partnerships, and coupling it with degree programs and research around healthcare quality, we can accomplish much more together than any single hospital can do alone.
We are starting to plan for a mental health initiative. There is no greater medical need in this region than mental health services and unfortunately, no need that is timelier. This program will be broad and ambitious. A third initiative will be a focus on research and programs related to cancer. We look forward to reporting on these efforts as they move forward.
TCMC was created by this community, many of our students are from this community, and our mission is to serve the community. We see 2013 as an “inflection point” with many of our growing pains behind us and tremendous opportunities for success and service ahead. We are excited for the future of the school, our students, and this region, and we hope that this excitement will be contagious.
Best wishes for a healthy and happy New Year.
Guest Columnist: Steven J. Scheinman, M.D., President and Dean, The Commonwealth Medical College
Read Dr. Mackarey’s Health & Exercise Forum – Every Monday in the Scranton Times-Tribune. The Next Two Mondays will feature TCMC 2nd Year Medical Student, Lani Hossain.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
