
Baseball Catcher Squat Position
Why write a column about baseball when the season is winding down? Well, baseball is NOT over yet! In fact, the season is just getting exciting as the playoffs are just around the corner. Also, for those not playing in the big leagues, “fall ball” and travel league is just getting under way. AND, by the way, the off season is the best time to work on specific conditioning…so stay fit and play safe!
In baseball, pitchers often receive all the notoriety and attention. Their shoulders are treated with tremendous care and attention…warm-up, pitch counts, protection and warmth in between innings, and cool-down with days of rest in between games. Catchers, however, who throw at least as many times (usually more) in a game as pitchers, receive much less attention to detail regarding their throwing shoulders. New research has found that, because catchers often throw off balance, the best way to protect a catcher’s shoulder is to strengthen his abdominal core and lower body muscles.
A catcher’s shoulder endures the same torture and torment of training and performance, but research remains limited on prevention of shoulder injuries specific to the position relative to pitchers. Because the majority of throwing injuries occur at the shoulder, conditioning programs typically focus on the shoulder girdle muscles. However, current wisdom from Auburn University researchers suggests shifting the training emphasis to the core and lower body. If the catcher’s lower body cannot support the dynamic movements of his upper body, the weakest link, the shoulder, will be sacrificed.
Most of the game a catcher will throw the ball back to the pitcher without too much velocity. However, as a catcher, throwing is often performed in a squatted or off balance position and creates tremendous stress on the shoulder. Additionally, a catcher must make a quick and ballistic throw to second or third base when a runner attempts to steal the base. Studies show that the stronger the abdominal core and lower body, especially the gluteals, the less likely the player is to develop shoulder injuries.
So, if you are a baseball catcher like Matt Hayes, or any throwing athlete, the best way to improve your skills and prevent shoulder injuries is to concentrate on a core abdominal and gluteal strengthening program:
Front Plank:
Front Plank on Bosu Ball:
Once isometric core stability exercises are mastered, you may begin gluteal strengthening
Static Clam:
Static Hydrant:
Static Side-Lying Abduction:
Static Squat With Band:

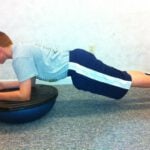




Photo Model: Matthew Hayes, Catcher for Moosic Mets Travel Baseball Team
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in Scranton, PA. He is an associate clinical professor of medicine at The Commonwealth Medical College.

Catherine Udomsak, SPT
Guest Contributor: Catherine Udomsak, SPT
Exploring Alternative Medicine: Acupuncture, Part 2 of 2
The majority of the public is familiar with traditional Chinese acupuncture, involving thin needles and specific body points. However, the practice of acupuncture offers great variety and distinctive techniques have developed over the years. As the practice spread throughout the world, countries expanded upon the traditional method and created new forms of acupuncture. The different types include but are not limited to:

Catherine Udomsak, SPT, administers noninvasive electro-acupuncture to patient model, Vanessa Borgia.
With all the different types of acupuncture available, you may be wondering, could I benefit from some form of treatment? A variety of ailments can be treated with traditional acupuncture andmany, who have been failed by conservative medicine, turn to this ancient practice for relief. Physical pain is a common complaint for Americans, and chronic pain can be a lifelong battle. According to the National Health Interview Survey, pain or musculoskeletal complaints accounted for 7 of the top 10 conditions for which people use acupuncture. Pain conditions included but were not limited to low back pain, headaches/migraines, neck pain, osteoarthritis/knee pain, carpal tunnel syndrome, menstrual cramps, myofascial pain, fibromyalgia, tennis elbow, TMJ dysfunction, rheumatoid arthritis, and even postoperative dental pain. While research confirms that acupuncture can be an effective treatment for chronic pain, it is still unclear as to which diagnoses benefit the most from treatment. Other conditions for which acupuncture has been used include; gastrointestinal disorders such as IBS, drug addiction, and psychiatric disorders including depression. The list of conditions continues, however, solid evidence to support its use is lacking. This is in part due to the fact that many different acupuncture techniques are in existence, making it challenging to compare studies. Furthermore, many studies suffer from methodological errors such as small treatment sizes and a lack of control groups. Nonetheless, certain individuals swear by this alternative treatment option.
If you are considering giving acupuncture a try, make sure to go to a certified practitioner and think about discussing the idea with your primary care physician. A healthcare practitioner may be able to give you more insight on this treatment and recommend a reliable acupuncturist. A licensed acupuncturist, or LAc, has received a degree/diploma from an accredited college and passed the national certification exams. Sometimes medical or osteopathic physicians, who have had specific training in acupuncture, will use it as an adjunctive technique. Furthermore, certain forms of acupuncture including non-invasive electro-acupuncture and acupressure, can be performed by a physical therapist as an addition to treatment.
While acupuncture has become a popular method to treat pain and other symptoms of illness, more research needs to be performed on the science behind acupuncture and its effectiveness. For the most part, the current research is inconclusive and it is difficult to say which patients will have the most success. However, if conservative treatment has failed you and you are in search of relief acupuncture may be the right choice for you! Acupuncture may not be the cure to any disease but it can certainly ease one’s symptoms and provide pain relief. This ancient treatment has survived the test of time and continues to be one of the most prevalent forms of alternative medicine used today.
Visit your doctor regularly and listen to your body.
Guest Contributor: Catherine Udomsak, SPT, Temple University, Doctor of Physical Therapy 2014. Catherine, a native of Clarks Summit, PA, is an intern at Mackarey & Mackarey Physical Therapy Consultants, LLC and is the 2013 recipient of the Dr. Paul Mackarey Physical Therapy Health Care Journalism Award.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
 Guest Contributor: Catherine Udomsak, SPT
Guest Contributor: Catherine Udomsak, SPT
Exploring Alternative Medicine: Acupuncture. Part 1 of 2
One of the most widely practiced and a controversial form of alternative medicine used today is acupuncture. Presently, I have several patients using this modality for a wide variety of indications including; smoking cessation, whiplash pain, headaches, spasms associated with multiple sclerosis, and lower back pain.
Catherine Udomsak, SPT
Traditional acupuncture technique involves inserting thin needles of varying lengths into the skin to relieve pain and other symptoms of illness. It is an ancient form of healing originating from China where it has been in use for over 2,000 years. In China, acupuncture is commonly accepted and is even believed to cure disease and illness. This practice is rooted in Traditional Chinese Medicine (TCM) and its theory is based on the concept that bodily functions are regulated by a vital life force known as “Qi”.
According to Traditional Chinese Medicine theory, channels known as meridians assist the flow of Qi, pronounced chee, throughout the body. TCM purports that there are 12 major meridians in the human body, which connect to the bodily organs and represent an internal system of communication between the organs. Along the meridians are various acupuncture points, or acupoints. Originally, there were only 365 acupoints corresponding to the number of days in a year. However, overtime the number of acupoints has greatly increased. According to Traditional Chinese Medicine theory, illness occurs when the energy flow along one or more meridians is blocked or out of balance. From a “purist” perspective, the traditional purpose of acupuncture is to restore the balance to the energy flow and thus alleviate sickness.
Although it was commonly used throughout China, the popularity of acupuncture declined in the 17th century and it became regarded as superstition. As knowledge of Western medicine spread throughout China, acupuncture continued to fall out of favor until it was outlawed in 1929. However in 1949, due in great part to a widespread shortage of modern medical practitioners, acupuncture and other forms of traditional medicine were reinstated as a means to provide health to the massive population. The spread of acupuncture to other countries took place over years and it traveled by different methods. Jesuit missionaries who visited China in the 16th century were the first to carry knowledge of acupuncture to Europe. The interest in acupuncture in America occurred in 1971. James Reston, a reporter accompanying president Nixon to China, received acupuncture after an emergency appendectomy and experienced symptomatic relief. His report to the US media resulted in widespread curiosity throughout the country and led to a team of US physicians making a tour to China to learn about the ancient practice. In 1972, the National Institute of Health gave its first grant to study acupuncture and the first legal acupuncture center was established.
Since the initial introduction of acupuncture in the US there has been a controversial debate over the effectiveness of acupuncture and the lack of solid scientific evidence. There have been a number of studies exploring the biomechanics behind acupuncture and unfortunately the exact science of how it works still remains unknown. Researchers have suggested several biological effects the may account for acupuncture’s effectiveness. These explanations include the release in the brain and spinal cord of chemicals that subdue pain and transmit messages to nerves and muscles. Studies suggest that the needle stimulation causes the release of endorphins and other neurotransmitters, which produce an analgesic effect. Other explanations include hormonal changes as well as increases in cerebral blood flow and immune function. Still, other researchers are not convinced and believe that acupuncture works via the placebo effect.
Although the science behind acupuncture remains foggy, the demand for it remains and supporters claim that acupuncture can be used to treat physical illness, especially pain and muscle spasms. In addition, acupuncture has even been used to treat addiction and mental illness. While most people only know of traditional acupuncture involving thin needles, there are many other methods used to deliver acupuncture. All techniques are designed to relieve pain and other symptoms of illness. Next week’s column will compare the different techniques and further explore who could benefit from acupuncture treatment.
Visit your doctor regularly and listen to your body.
Guest Contributor: Catherine Udomsak, SPT, Temple University, Doctor of Physical Therapy 2014. Catherine, a native of Clarks Summit, PA, is an intern at Mackarey & Mackarey Physical Therapy Consultants, LLC and is the 2013 recipient of the Dr. Paul Mackarey Physical Therapy Health Care Journalism Award.
NEXT MONDAY – Read Acupuncture – Part 2; Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Frequently, patients ask for a home exercise program that is quick and easy. For some, they want to do some exercises before or after work to gain or maintain muscle tone, but don’t have time to join a gym. For others who are retired, they want to do some simple exercises to help them maintain independence and safety performing daily activities around the house such as; climbing stairs, getting in and out of a shower, putting on shoes and socks, cooking, cleaning, and carrying groceries or laundry. I have comprised 10 simple exercises including upper and lower body and balance and core. The only equipment you will need is a chair and resistance bands; yellow has the least resistance, black the most, red, green, blue in between. They can be purchased at any sporting goods or department store.
Remember, for most people it is more harmful not to exercise, so contact your physician to discuss whether independent exercise is appropriate for you. If you have special needs, you may need to consult with a physical therapist to get started.
These exercises are performed while sitting in a chair with backrest, slowly and hold the position for 3 seconds, 5 -10 repetitions, and 3-5 times per week. Begin with a yellow light resistance band.
Row the Boat
Saw Wood
Elbow Extension
Hip Spread
Hip Hike
Leg Kicks






Shoulder Shrug
Elbow Bend
Standing Leg Curl
Standing Walk Aways - Backward
Standing Walk Aways - Forward




Visit your doctor regularly and listen to your body. Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
A few months ago, I wrote a column entitled, “How do you know when you are ready for a new knee?” I received several emails with requests for more information regarding hip and knee replacements such as, outcomes, complications, etc. Some readers wanted to know about heart disease and joint replacements. One reader wanted to know about outcomes for obese patients. Another was concerned about the ability to return to work following a joint replacement. And, one reader asked about the special knee replacement made just for women. Research on these topics and others were presented at the American Academy of Orthopedic Surgeons 2013 Annual Meeting in Chicago. But, while research is valuable, please keep in mind that each person is unique and there is no substitute for productive discussions with your primary care physician and orthopedic surgeon.
A recent study looked back and examined more than 43,000 patients with osteoarthritis of the hip from 1998 to 2009. They discovered that, in addition to the well known short term benefits of joint replacement, there are many surprising long term benefits. Short term, it is known that joint replacements improve quality of life with reduced joint pain. Long term, they discovered that patients who had a total hip replacement had a lower mortality rate than those without replacements. These patients also had a lower risk of diabetes and depression. Researchers concluded that the long term benefits may be due to increased activity with less pain and improved mobility. The more active lifestyle may contribute to longevity and quality of life.
8,000 joint replacement patients were studied for differences in outcomes and complications between those who were obese and non-obese. Long term outcomes such as pain, range of motion, and quality of life were similar. Also, complication rates among obese patients were not higher if the patients did not have additional medical conditions, often associated with obesity, such as diabetes and high blood pressure. However, if these additional problems were present, then obese patients experienced longer and more expensive hospital stays and increased infection rates. Despite this, long term outcomes were satisfactory.
Due, in part, to an increased number of younger, working-age patients, receiving total joint replacements, researchers wanted to know if they were able to return to preoperative employment. 98% of patients with total knee replacements returned to previous employment for those employed three months before surgery. The return rate was as follows: 92% for sedentary, 79.% for light, 89.% for medium, 87.% for heavy and 78.% very heavy jobs.
Return to lifestyle was also explored. Before surgery, almost 40% of the patients reported an active lifestyle. Post surgically, an additional 16% of the patients were active. It was concluded, those who were active before surgery will return to activity and many others will regain an active lifestyle in activities such as; bowling, golfing, walking, and swimming. Additionally, many active patients return to more vigorous activities such as golfing, biking, hiking, tennis and skiing and hiking.
60% of all knee replacements occur in women and the female knee is shaped slightly different than that of a male. However, it has not been confirmed that the new “gender specific” knee replacement improves outcomes. In a large study group, while it was determined that the gender specific knee group appeared to have a better fit on follow-up x-ray, there were no differences in knee range of motion, pain, or function. Researchers concluded, at this time there are no disadvantages to the gender specific knee replacement and choosing the right size implant for the specific patient, regardless of gender, is important for positive outcomes. Therefore, the gender specific knee replacement provides more choices for the surgeon and patient to determine the best fit for the best possible outcome.
SOURCE: American Academy of Orthopedic Surgeons 2013 Annual Meeting in Chicago.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 2 of 2
After a long cold and rainy spring, NEPA is finally experiencing hot summer weather! So, get outdoors and have fun in the sun. However, please be mindful of how your body reacts to high humidity and heat and take appropriate precautions. You don’t have to be running a marathon or playing football in full uniform to suffer from heat stroke.
Heat stroke, one of the most serious heat-related illnesses, is the result of long term exposure to the sun to the point which a person cannot sweat enough to lower the body temperature. The elderly and infants are most susceptible and it can be fatal if not managed properly and immediately. Believe it or not, the exact cause of heatstroke is unclear. Prevention is the best treatment because it can strike suddenly and without warning. It can also occur in non athletes at outdoor concerts, outdoor carnivals, or backyard activities.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 1 of 2
After a long cold and rainy spring, NEPA is finally experiencing hot summer weather! So, get outdoors and have fun in the sun. However, please be mindful of how your body reacts to high humidity and heat and take appropriate precautions. You don’t have to be running a marathon or playing football in full uniform to suffer from heat stroke.
Heat stroke, one of the most serious heat-related illnesses, is the result of long term exposure to the sun to the point which a person cannot sweat enough to lower the body temperature. The elderly and infants are most susceptible and it can be fatal if not managed properly and immediately. Believe it or not, the exact cause of heatstroke is unclear. Prevention is the best treatment because it can strike suddenly and without warning. It can also occur in non athletes at outdoor concerts, outdoor carnivals, or backyard activities.
Some “old school” folks think that wearing extra clothing and “breaking a good sweat” is an optimal goal for exercise. However, it may be potentially very dangerous in hot and humid conditions. When exercising in hot weather, the body is under additional stress. As the activity and the hot air increases your core temperature your body will to deliver more blood to your skin to cool it down. In doing so, your heart rate is increased and less blood is available for your muscles, which leads to cramping and other more serious problems. In humid conditions, problems are magnified as sweat cannot be evaporated from the skin to assist in cooling the body.
The American Academy of Pediatrics and The American College of Sports Medicine has the following recommendations which are appropriate for both the competitive athlete and weekend warrior:
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune Next Week: “Heat Stroke Part 2"
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email:drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
Prevention of Shoulder Injuries In Tennis by Stretching
Part 2 of 2
Last week we discussed the importance of strengthening to prevent shoulder injuries in tennis. This week we will focus on stretching the shoulder for injury prevention. As with the exercises for strength, it may be better to do nothing at all than to do so improperly. For example, the shoulder must be adequately warmed up and in the proper position and alignment to fully benefit from stretching. New research is demonstrating that proper stretching to promote good posture may help or even prevent shoulder problems.
Part of the rotator cuff, a group of muscles that stabilize the shoulder, passes between the arm bone (humerus) and a bone in the back (scapula). Due to the nature of the overhead tennis stoke or overuse from constant hitting, the rotator cuff can be repetitively pinched between the two bones. This produces a painful inflammatory condition known as rotator cuff tendonitis of the shoulder.
If the shoulder blade is tipped downwards, such as the position the shoulder assumes when slouching, it will place the shoulder in a position which pinches part of the rotator cuff. Stretching, strengthening or hitting a ball in this position will ultimately lead to problems. Add excessive training and practicing to the mix and this overuse may cause the muscles and tendons of the rotator cuff to become inflamed and swell. The swelling of the muscles and tendons will make the shoulder more prone to impingement.
A tight neck, chest and muscles in the front of the shoulder may cause a tennis player to assume a hunched over posture. This poor posture decreases the distance between the humerus and scapula making the shoulder more prone to impingement. Good posture with head and shoulders back increases the distance between the humerus and scapula. Therefore, proper stretching and good posture is important for prevention of shoulder pain because it decreases the impingement.
Warm Up: Never stretch a cold muscle because the muscle can tear instead of stretch. To warm up the muscle one can run or jog for 5 minutes, place a heating pad on the area to be stretched, slowly move the arms in the direction that imitates various tennis strokes at 25-50% speed (dynamic stretching) while never moving far enough to cause discomfort. After practice, one can perform stretches that are more aggressive and held for 5-10 seconds with slight discomfort to improve flexibility. Aggressive stretching before competition may weaken the muscle and effect performance.
The Nicholas Institute of Sports Medicine and Athletic Trauma suggests the following stretches to be performed actively (dynamic) without discomfort to 90% range of motion before competition and passively and hold to 100% end range of motion (static) with slight discomfort after practice.
Triceps Stretch: Begin by raising your arm directly over your head. Bend your elbow and try to reach the shoulder blade on the same side of you body. Use your opposite arm to push your elbow back.
Corner Stretch to the Pectoralis Major: Begin by facing a corner and placing your forearms on the wall at a 90 degree angle. Step forward with one foot to feel the stretch.
Infraspinatus Stretch: Extend your arm out directly in front of you and bend your elbow across your body. With your other hand gently pull your elbow across your body.
Latissimus Dorsi Stretch: Raise both arms overhead and place palms together interlocking fingers. At shoulders, lift arms upwards with fingers remaining intertwined.
Head Over Shoulders: Pull your chin down and backwards as if trying to make a double chin.
Shoulder Blade Pinch: Pinch shoulder blades together
Standing Extension: Stand and lean backwards - extend lower back.







Contributor: Gary E. Mattingly, PT, PhD: Professor, University of Scranton, Dept. of Physical Therapy, Shoulder Rehab Specialist, Mackarey & Mackarey Physical Therapy
Models: Katherine Weaver, Amanda Brown
Keep in mind that avoiding bad posture in your day to day activities can help keep your shoulder and back healthy, so remember “Sit up straight!”
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Prevention of Shoulder Injuries in Tennis
Part 1 of 2: Strengthen to Prevent Shoulder Injuries in TennisYou can tell that it is officially summer, not only by the arrival of the longest day of the year, but also by the beautiful sound of a tennis ball hitting a racquet hitting at Scranton Tennis Club and Birchwood Racquet and Fitness Club. So, get your racquets out and join the fun! However, take time to “tune up” in order to prevent injury, especially to the shoulder. In a sport that relies so heavily on the use of the shoulder, it is very common for tennis players to develop occasional shoulder pain or a more chronic problem such as shoulder rotator cuff tendinitis. That is exactly what happened to professional tennis star, Maria Sharapova and many others over the past few seasons.
For many, tennis is more of a seasonal sport. For example, in high school it is played in the fall for girls and spring for boys. In the off-season, a shoulder can lose much of its essential strength. This loss will result in a deconditioned shoulder at the start of the season and making it more susceptible to injury. Practicing with a deconditioned shoulder commonly results in sprain, strain and pain. Pain and weakness will significantly interfere with the ability to perform at a high level.
To prevent shoulder problems one must participate in an exercise program specifically designed for tennis. A well-balance shoulder strengthening program includes; rotator cuff and scapular (shoulder blade) muscle exercises, reeducation, biomechanics, and a stretching program pre and post hitting. This column will discuss some of these principles to properly prepare your shoulder for the tennis season and avoid injury.
To avoid shoulder pain it is necessary to maintain shoulder strength. Stretching exercises are also important and will be discussed in next week in, Prevention of Shoulder Injuries in Tennis - Part II. Strengthening exercises need to concentrate on three groups of muscles: power muscles (the large muscles of the shoulder), shoulder blade stabilizer muscles (the muscles which stabilize the shoulder blade, and the all important rotator cuff muscles (the muscles which move the shoulder and control the cocking and follow through phases of the tennis stroke, while keeping the joint in proper position). Strengthening the power muscles of the shoulder is fairly easy; latissimus pull downs, pectoralis bench presses, and bicep curls will cover all bases. While these exercises are important in maintaining strength and power of the throwing shoulder, they are not as important as the exercises for the shoulder stabilizers and rotator cuff muscles.
Rotator Cuff Internal Rotation (Tennis Forehand Stroke)
Holding a light or medium resistance band, imitate a forehand stroke with slight bend in the elbow.
Rotator Cuff External Rotation (Tennis Backhand Stroke)
Latissimus Pull downs – Kneeling or sitting
Bench Press - Lying on back with knees bent
Biceps Curls - Sitting or standing





Model: Catherine Weaver
Visit your doctor regularly and listen to your body.
Contributor: Gary E. Mattingly, PT, PhD: Professor, University of Scranton, Dept. of Physical Therapy, Shoulder Rehab Specialist, Mackarey & Mackarey Physical Therapy
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune. Part II “Prevention of Shoulder Injuries in Tennis”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
REFLEX SYPATHETIC DYSTROPHY - TREATMENT
Part 2 of 2
The focus of last week’s column on reflex sympathetic dystrophy (RSD) was cause and diagnosis. This week we will discuss treatment and prognosis. The cornerstone of RSD treatment is normal use of the affected part. Therefore, all modalities are employed to facilitate movement:
The prognosis for RSD varies. For some, complete recovery occurs and symptoms are minor. However, some people experience spontaneous remission, while others can have unremitting pain and crippling, irreversible changes. The longer RSD is left without direct medical intervention, the more difficult it is to treat. More research is needed to understand the causes, progression and the role of early treatment.
For More Information:
Contributor: Janet Caputo, PT, DPT, OCS; Clinic Director at Mackarey & Mackarey Physical Therapy Consultants, LLC in Scranton, PA.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
