 Michael Vick injured his hamstring muscle in early October and after 3 weeks of rest, he attempted to return lead the Eagles against the Giants on October 28. Unfortunately, he was not ready to return and was reinjured. I have a confession to make…I am an Eagles fan! God help me! As such, I am painfully aware of the inability of the Eagles high speed offense to perform successfully without Vick. And, I am also painfully aware of Vicks inability to perform in this offense without a healthy hamstring. Time to answer a few commonly asked questions…What is the hamstring? How is it injured? What is the best treatment?
Michael Vick injured his hamstring muscle in early October and after 3 weeks of rest, he attempted to return lead the Eagles against the Giants on October 28. Unfortunately, he was not ready to return and was reinjured. I have a confession to make…I am an Eagles fan! God help me! As such, I am painfully aware of the inability of the Eagles high speed offense to perform successfully without Vick. And, I am also painfully aware of Vicks inability to perform in this offense without a healthy hamstring. Time to answer a few commonly asked questions…What is the hamstring? How is it injured? What is the best treatment?
A hamstring strain is a tear of the muscle fibers of the muscle group in the back of the thigh called the hamstring. The hamstring muscle is a group of three muscles that run from the back of the hip (lower pelvis), crossing the back of the knee and attaches to the knee bone (tibia). The hamstring muscles work to extend the hip and bend the knee during running and walking activities. They are very active when an athlete changes direction, especially forwards and backwards or decelerating. This injury, like others muscle strains, varies in intensity. Severe hamstring strain occurs when many muscle fibers are torn. The athlete may experience a sudden onset of severe pain in the back of the thigh and occasionally report a popping sensation. Pain, swelling and black and blue skin from tissue damage and bleeding is often reported. Pain in increased when attempting to bend the knee. In very severe cases, the boney attachment can be pulled so strongly that a small fracture can occur. Healing time can be as short as a few days or as long as weeks or even months.
Your family physician will examine the back of your leg to determine if you have hamstring strain. Sometimes, pain in the buttocks and back of the leg can be referred from you lower back if the sciatic nerve is inflamed. In more advanced cases, you may be referred to an orthopedic surgeon for further examination and treatment. An X-ray, MRI or bone scan will show the extent of the tear and if the bone is involved. The diagnosis will determine if your problem is minor, moderate or severe.
There are many conservative options. Your family physician or orthopedic surgeon will help you decide which choices are best.
Recent studies have determined that a training program specifically designed to prevent hamstring injuries is effective, especially for the competitive athlete. This program includes:
SOURCES: Journal of Physical Medicine & Rehabilitation and American Academy of Orthopaedic Surgeons
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum" in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Guest Columnist: Lani Hassani, 3rd Year Medical Student, TCMC
On Saturday, November 16, 2013, The Commonwealth Medical College (TCMC) will hosted a symposium on substance abuse for health care providers in NEPA. The following column on current research regarding the neurology of self-control and substance abuse was written on by Lani Hassani, 3rd year medical student at TCMC.
A recent study from the University of Iowa led by neuroscientist William Hedgcock has shown through functional magnetic resonance imaging (fMRI) that the brain has no trouble consistently recognizing temptations. However, the brain’s self-control components can in fact be used to the point of exhaustion, contrary to the prior belief that self-control can be strengthened through repetitive use. The study purports that once self-control stamina has been depleted, the brain will have a harder time regulating activity to avoid the red-flagged temptations. The researchers termed this phenomenon “regulatory depletion”.
“I know I really shouldn’t, but I’m going to anyway,” is a phrase that may indicate you are experiencing self-control fatigue. It is also relevant to note that self-control is separate from impulsiveness. While the self-control portions of the brain stop a person from completing a certain action due to long-term consequences, impulsive behavior is positively motivated by small, immediate rewards. For example, stealing a piece of candy from a coworker’s desk to satisfy a craving would be impulsive behavior. The immediate reward is the candy. Not eating the sweet, stolen loot is self-controlled behavior because the thought of extra dietary calories, cavities from the sugar, and repercussions from the candy’s prior owner are all consequences that would deter the impulsive behavior.
Hedgcock’s revelation means that testing ones’ self-restraint does not build stronger powers of avoidance and can actually be detrimental. Say the sweet-toothed thief had recently quit smoking and had braved lunch in a smoky bar just an hour earlier. The self-restraint regions of his brain would already be burned out from battling tobacco cravings, so he would be a lot more likely to give in to his sugar cravings and eat the piece of candy.
What does this mean for me?
Because the one part of the brain fatigues while the other remains strong, there is no change in how we perceive temptation and relate it to our short and long term goals. Yet, relying solely on self-control to eat healthily or quit smoking can mean disaster when stress and repetition have literally chemically and metabolically exhausted the brain’s willpower.
When it comes to healthy habits, the right kind of motivation can help overcome self-control fatigue, says a 2012 review in the International Journal of Behavioral Nutrition and Physical Activity.
Identify the conflict and modify the behavior
Guest Columnist, Lani Hassani, is a 3rd Year Medical Student at The Commonwealth Medical College (TCMC) where she plans to practice family medicine in an underserved region. She was born in Switzerland and has lived on both coasts of the US. Lani received her undergraduate degrees in Environmental Science and Anthropology from the University of Virginia, where she was also the section editor of the university paper’s Health and Science section. She is currently the president of TCMC’s Healthcare in Journalism Club and one of four class officers. When she needs a break from studying, Lani loves to do anything outdoors, travel, and cook for her friends.
Read “Health & Exercise Forum” – Every Monday in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Guest Columnist: Janet Caputo, PT, DPT, OCS
Peripheral arterial disease (PAD), also known as peripheral vascular disease, is an obstruction or narrowing of the large arteries, usually in the legs. These narrowed or clogged arteries cause a lack of blood flow to your body’s tissues (i.e. muscles, tendons, ligaments, nerves, etc.). It can be caused by atherosclerosis or inflammation which may lead to stenosis and complicated by associated embolisms, similar to what occurs in the smaller arteries of the heart and brain. It can be painful and debilitating. It typically affects 12-14% of the general population, however, it is found in 20% of those over 75.
Have you seen the commercials on television for peripheral artery disease (PAD) recommending laser, electrical stimulation, or ultrasonic sound waves to alleviate symptoms? While tempting, there is little to no scientific support for these treatments. Reliable sources, such as the American College of Cardiology and American Heart Association, advocate EXERCISE as the best treatment for PAD.
Research has identified several factors that increase your risk for developing PAD. You can control many, but not all, of these risk factors. The uncontrollable risk factors include:
However, be optimistic and focus on the following controllable risk factors:
PAD affects men and women equally and is often associated with coronary artery disease (AKA: heart disease) which can cause a heart attack and cerebrovascular disease which can cause a stroke. To reduce your risk of heart attacks and stroke, anti-coagulant therapy is recommended, with aspirin as the first choice.
PAD symptoms can interfere with your ability to maintain an active lifestyle. This lack of “exercise” decreases your balance, strength, endurance, and walking ability. You may succumb to a sedentary lifestyle which reduces quality of life and increases risk for disability and death! Therefore, PAD requires aggressive management!
Proper management of PAD includes reducing not only the risk factors, but also the pain that you experience with activity! The American Heart Association and the American College of Cardiology recommend a supervised exercise program because:
The American College of Cardiology and the American Heart Association endorse a walking program, 30 to 45 minutes in duration, at least 3 times per week, for at least 12 weeks. Other components of the ideal walking program need to be identified by a medical professional:
In more severe cases of PAD, revascularization with surgical techniques should be considered if the above mentioned conservative measures have failed. Please consult with your doctor before beginning any exercise program!
Visit your doctor regularly and listen to your body.
CONTRIBUTING AUTHOR: Janet Caputo, PT, DPT, OCS is clinical director of physical therapy at Mackarey & Mackarey Physical Therapy Consultants, LLC in downtown Scranton where she practices orthopedic and neurological physical therapy.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in Scranton, PA. He is an associate clinical professor of medicine at The Commonwealth Medical College.

Gina Tomaine
Guest Columnist: Gina Tomaine
I decided to train for my first marathon shortly after running a ten-mile road race in Washington D.C. in spring of 2013. I had been running 5Ks for about a year at that point, and my overall health and fitness was at an all-time high. Not only was my fitness commitment strong, but I also was looking for a goal to build towards to motivate me mentally and physically to improve. I had been living in Boston for three years, and cheering for runners at the Boston Marathon each year made me fall in love with the marathon distance. After the bombing at the 2013 Boston Marathon, I only wanted to run more. I wanted to honor the legacy of so many that had run that marathon, by continuing that spirit of determination, strength, and joy.
I chose the Steamtown Marathon because it was an ideal fall marathon. I loved the linear nature of the race, and also, that it was a hometown race. It seemed positive and symbolic to be able to literally run home. My training plan consisted of short to mid-length runs during the week and a long-run every weekend, usually every Sunday. I started building up from my ten-mile run back in the spring by adding 1-2 miles each weekend. I would run 10 miles one weekend, the following weekend 13, and the following weekend 15, and so on, ending at around 20 or 22 miles at three weeks before the marathon.
In addition to my long runs every weekend and short runs during the week, I cross-trained heavily to work on different muscle groups and stay balanced. I practiced Vinyasa and Bikram yoga 1-2 times a week. For a different cardio workout, I substituted a short run with Zumba, Kickboxing, and the elliptical. The yoga always made me feel more limber and at ease with my running, the different cardio routines kept my body adaptable and in shape, and the elliptical was a big help to my knees and feet when I needed a lower-impact workout. I also made sure to incorporate strength and resistance training with some lightweight (5 pound) weights, squats, lunges, as well as regular planks, sit-ups and abs workouts.
In August and September of my training, I started to feel pain in my knees and hips, as well as my foot. I started incorporating physical therapy into my routine with exercises given to me by my local physical therapist, Dr. Mackarey. These exercises helped to strengthen my knees and hips to handle the intense strain put on them by all the mileage I was putting in. With regular exercise, therapy, heat, ice, stretching, foam-rolling, and continuing to include yoga in my weekly routine, my knees held up.
On race day I was terrified and excited, and made sure to do everything I had normally done during my race routine. The cannon blasted, and I started out pacing myself with the hills in Forest City. It was difficult to hold back with all the adrenaline, but my training reminded me to save my energy for the end of the race. All the support from family and friends, clever and encouraging signs (“I’m proud of you, perfect stranger!”), and free distribution of orange slices and bananas throughout the valley were nonstop encouragement as I made my way towards Scranton. I felt strong and sure that I could complete the race, and my goal as a first-timer was simply to finish under 5 hours.
At around mile 20 I started to lose heart. The pain of repetitive exercise in my joints was starting to overwhelm my mental drive to finish, and it was difficult, most of all, to keep focus. I knew I couldn’t stop, with all the crowds and the other runners there. I knew I had to finish, and that instinct took over. With encouragement from friends, I kept going, and kept a steady running pace up the hills of both the Boulevard and Electric St. The shouts and music blasting in Green Ridge were a huge mental pick-me-up, and also meant the race was almost finished.
Even at mile 25, I felt like I didn’t know how I was going to make it down the final stretch. But that drive, that willpower, and that joy of the race prevailed, and I kept moving past Cooper’s, down North Washington, and towards Courthouse Square. When I saw the bright finish line sign, my heart filled up. I sprinted the last two blocks with a burst of energy I didn’t know I had. I raised my arms in the air as I crossed the tape of the finish line, received a medal around my neck, a Mylar blanket around my shoulders. I was a marathoner.
Guest Columnist: Gina Tomaine, MFA Emerson College 2013, is a freelance writer and editor whose work has appeared in The Philadelphia Inquirer, The Boston Globe, and Boston Magazine. She is a Dickson City native and avid runner.
Read Dr. Mackarey’s Health & Exercise Forum – Every Monday in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Scoliosis Part 2 of 2. Idiopathic And Adult Scoliosis.
Scoliosis is a term used to describe a curvature of the spine. This two part series on scoliosis will discuss scoliosis, diagnosis, and treatment at the request of several readers. Scoliosis screening is very important for early intervention and prevention of long term and irreversible problems.
Idiopathic adolescent scoliosis is a structural scoliosis. It has strong genetic tendencies and is the most common type of scoliosis. There is abnormal sidebending of the spine in an otherwise healthy child. The cause remains unknown! General characteristics are as numerous. The scoliosis often manifests after puberty, 80% are 11-14 year old females with rapid curve progression during the growth spurt. Also, it is more common among taller than average girls with an earlier growth spurt, longer growth period and advanced skeletal age. It is associated with an increased level of growth hormone and may have associated postural, equilibrium, and vestibular dysfunctions.
The progression of the curve is determined by several factors a more rapid curve progression is noted in females with a rapid rise in progression at the onset of the adolescent growth spurt. It is less common after menarche and after a sign of skeletal maturity (Risser Sign). Double curves progress more frequently than single curves and curve magnitude increases in larger curves.
To develop a comprehensive treatment approach, a thorough musculoskeletal evaluation must be performed. This may include assessments from a variety of medical professionals and various imaging studies. Observation with repeat x-rays to determine progression is the first phase in addressing adolescent idiopathic scoliosis. The rest of the treatment course may progress as follows:
I. Non-operative Treatment Progression
A. Electrical stimulation (LES)
1. to the muscle on the convex side of the curve
2. less effective than bracing
B. Bracing
1. May prevent 74 – 81% of the curve from worsening
2. Most effective in curves between 25–35 degrees
3. General guidelines:
a. if < 20 degrees and skeletally mature, bracing is not recommended
b. if < 30 degrees, but progresses > 5 degrees over 12 months, bracing is required
c. if > 30 degrees brace immediately
4. Effectiveness is time dependent(worn 23 hours per day)
5. Worn until skeletal maturity
II. Operative Treatment Progression
A. Operative Treatment is indicated if
1. curve > 50 degrees and skeletally mature
2. curve > 30 degrees with marked rotation
3. double major curves of > 30 degrees
B. Options for surgical intervention
1. Segmental Instrumentation
2. Instrumentation with fusion with either casting or bracing until fusion solid (4 to 8 months)
Adult scoliosis is another type of structural scoliosis. The adult curves may progress more slowly. There are two types. One, is associated with an original onset before skeletal maturity. The second type arises early in adult life due to:
1. Osteoporosis (decreased bone density) which causes compression fractures that have a major role in scoliosis progression in post menopausal women. Therefore, in pre-menopause perform 20 minutes of general low-impact aerobics 4x/week and in post- menopause consider adding hormonal therapy and calcium.
2. Osteomalacia: decreased bone formation, decreased bone mass, and Vitamin D deficiency
3. Iatrogenic: multiple level decompressions secondary to spinal stenosis or degenerative changes
When adult scoliosis progresses, the individual may notice:
1. Change in the way clothes fit
2. Increased rib hump
3. Loss of height
4. Loss of waist line
Non-operative management of adult scoliosis can decrease pain, increase function, but can not stop progression. These treatments include:
If there is significant curve progression, neurologic problems, increased disability, pain that significantly impacts daily activities, surgery may be recommended. Cosmesis is another reason for surgical intervention in adult scoliosis. The procedure of choice is usually instrumentation with fusion.
In summary, your physical therapist can assist in treating scoliosis by providing a thorough screening evaluation, designing an appropriate therapeutic exercise regimen, and offering pain management. If needed, the therapist can also develop the post-operative reconditioning program. The cost of bracing and surgery are comparable, but when screening is combined with bracing, the total cost decreases. In the end, the key to treating scoliosis is early detection and intervention.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
Contributor: Janet Caputo, PT, DPT, OCS is clinical director at Mackarey & Mackarey Physical Therapy Consultants, LLC. in downtown Scranton where she specializes in orthopedic and neurological rehab.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum" in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Scoliosis: Part 1 of 2. Functional Scoliosis.
Scoliosis is a term used to describe a curvature of the spine. This two part series on scoliosis will discuss scoliosis, diagnosis, and treatment at the request of several readers. Scoliosis screening is very important for early intervention and prevention of long term and irreversible problems.
The spine has three regions: the neck, the upper back, and the lower back. Each region normally curves in a particular direction. The neck and lower back curve inward (lordosis). The upper back curves outward (kyphosis). However, with scoliosis, the spine curves abnormally in a sideways direction greater than 10 degrees. This lateral flexion of the spine is also combined with a twisting or rotation of the vertebrae. Scoliosis can affect any of the three spinal regions and any age group.
There are a number of anatomic changes that occur with scoliosis. The sideways curve of the vertebrae produces a concavity (inward curve) on one side of the spine and a convexity (outward curve) on the opposite side. On the concave side of the curve, the ribs approximate, the intervertebral discs are compressed, disc spaces are narrowed, and the trunk muscles are shortened. On the convex side of the curve, the opposite occurs. The twisting of the vertebrae that accompanies the sidebending causes the ribs to deviate. On the concave side, the front ribs are pushed forward and on the convex side, the back ribs are pushed backward. This is responsible for the characteristic rib “hump” on one side of the back. With scoliosis there may be two curves present: one major curve which is usually considered “structural” (i.e. permanent changes in the shape of the bone and/or tone of the muscles) and one minor curve which is a compensatory curve to balance the trunk and allow it to be upright.
In the literature there are two types of scoliosis: functional and structural. A functional scoliosis is not produced by abnormal bone development or muscle tone. The causes are varied and may include:
1. Nerve root irritation (sciatica).
2. Muscle spasm due to spinal injury.
3. Poor posture.
4. Highly repetitive, asymmetric activities related to hand dominance.
5. Leg length discrepancy caused by a true shortening of the limb or compensatory secondary to faulty lower limb alignment.
A functional scoliosis is easily corrected once the cause is determined. Once nerve root irritation and muscle spasm dissipate, the scoliosis will resolve. Poor posture, hand dominance, and leg length discrepancies can lead to muscle imbalances (certain muscles shorten and others lengthen) resulting in a functional scoliosis. Be aware of poor postural habits! If a particular posture is assumed in a variety of positions throughout the day (sitting, standing, laying), you are prone to develop muscle imbalances that may lead to scoliosis. Hand dominance causes an individual to frequently assume certain postures and positions throughout the day. When sitting, there will be more weight on one hip than the other. This individual will lie on one side more often in order to allow use of the dominant hand to turn the pages of a book or to write. Also, objects will be carried on one side more than on the other. An individual with a leg length discrepancy will stand with body weight shifted onto one leg or will stand with one knee bent. If not addressed, a functional scoliosis may produce abnormal permanent changes in the bones and muscles.
Treatment for a functional scoliosis includes exercise to stretch the short muscles and to strengthen the long muscles. This will usually correct the muscle imbalances to prevent further exaggeration of the curve. Exercises are carefully selected on the basis of a thorough examination. Adequate instruction ensures precise performance. Researchers advocate educational programs in public schools for postural awareness due to the high incidence of poor postural habits. Additional supports in the form of orthotics for flat feet and heel lifts for leg length discrepancies can be used to assist in the treatment of scoliosis. The combination of the correct exercises, precise performance, and education on avoiding habitual positions, postures, and activities that may accentuate the curve should remedy the functional scoliosis.
Over the next two weeks, two common types of structural scoliosis will be discussed.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
Contributor: Janet Caputo, PT, DPT, OCS is clinical director at Mackarey & Mackarey Physical Therapy Consultants, LLC. in downtown Scranton where she specializes in orthopedic and neurological rehab.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune entitled “Scoliosis - Part 2”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Steamtown Marathon is quickly approaching…
This is the time of year when local runners are ramping up their training for the marathon or gearing up for high school cross country. It is also the time of year when many runners come to our clinic with shin splints. Many of these athletes are female runners, however, to a lesser degree soccer and football players, cheerleaders and dancers can get them too. Unfortunately, in many of these athletes, this problem can lead to a much more severe and advanced problem with shin splints called a stress fracture. Some very good athletes have been hindered by this problem. Some of the questions they and other patients have had regarding this problem are:
A stress fracture is fatigue damage to bone with partial or complete disruption of the cortex of the bone from repetitive loading. While standard x-rays may not reveal the problem, a bone scan, and MRI will. It usually occurs in the long bones of the leg, mostly the tibia but also the femur (thigh) and foot. Occasionally, it occurs in the arm.
10-21% of all competitive athletes are at risk for stress fractures. Track, cross country and military recruits are at greatest risk. Females are twice as likely as males to have a stress fracture. Other athletes at risk are: sprinters, soccer and basketball players, jumpers, ballet dancers are at risk in the leg and foot. Gymnasts are also vulnerable in the spine while rowers, baseball pitchers, golfers and tennis players can experience the fracture with much less frequency in the ribs & arm.
The problem is much more prevalent in weight bearing repetitive, loading sports in which leanness is emphasized (ballet, cheerleading) or provides an advantage (distance running, gymnastics).
Stress fractures usually begin with a manageable, poorly localized pain with or immediately after activity such as a shin splint. Over time, pain becomes more localized and tender during activity and then progresses to pain with daily activity and at rest.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email:drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
September is National Childhood Obesity Month. Obesity in America has become an epidemic and in contemporary society, this problem cannot be effectively addressed without recognizing the impact of computer technology on obesity. Computer technology has made our lives much easier. Computers allow us to communicate with each other faster, book vacations, shop in stores, visit the library, and develop photographs. Ancient Chinese culture would warn that this positive “Yang” must have a negative “Yin”. Recent studies have shown that excessive use of electronic devices (i.e. computers, cell phones, electronic books, etc) contributes to childhood obesity and a host of other problems such as computer vision syndrome.
Childhood obesity has more than tripled in the past 30 years. Obesity in children from 1980 to 2008 has increased from 6.5% in 1980 to 19.6% in 2008 in children between 6 to 11 years of age and from 5.0% to 18.1% in adolescents between 12 to 19 years of age. Childhood obesity is associated with increased cardiovascular risk in adulthood for heart attack and stroke. Obesity results from not only our heredity but also from the amount of physical activity or exercise that we do or are encouraged to do. Obesity results from an imbalance between the amount or quality of food we eat and the amount of physical activity or exercise we perform.
Since childhood obesity is linked with physical inactivity, increasing regular exercise is an important component in preventing obesity. As parents, we must consider alternatives to our children’s computerized pursuits and encourage them to engage in physical activities. Adults must be good role models regarding healthy eating and regular exercise. Consider planning an active family vacation with activities that involve hiking, biking, kayaking, white water rafting, and mountain climbing. Encourage children to participate in scholastic or intramural sports including baseball, softball, football, soccer, skiing, tennis, and golf.
Unfortunately, many of today’s children are on some type of computerized device almost all day. If they are not communicating with their friends online, then they are texting them on their cell phones. If they are not completing a homework assignment online, then they are reading their electronic book. It’s not only the teenagers, but also elementary and preschool children.
Introducing children to computers has improved their academic achievement. Studies show that children who used computers excelled in their levels of attention, memory, language development, comprehension, problem solving, and decision making, when compared to children who did not use computers. Children who did computer work both at home and at school performed better than those who did computer work only at school.
However, you know what “too much of a good thing” causes…harm! In addition to obesity, many eye care practitioners who specialize in children’s vision believe that prolonged computer use among children puts them at risk for progressive nearsightedness. To see clearly, the eyes have to focus. Focusing requires the use of our eye muscles. Use of any muscle strains the muscle and the muscle becomes tired and fatigued. Excessive use of any muscle causes muscle damage and injury. Some vision specialists believe that eye muscle fatigue caused by excessive focusing can lead to changes within the eye that cause nearsightedness. Experts agree that focusing on images on a computer screen causes greater eye fatigue than reading normal print in a book/ magazine or even watching a television program.
As parents, we must teach our children how to balance their yins and yangs. To reduce the likelihood of obesity, limit constant use of computer technology and encourage regular physical activity and healthy eating. To reduce eye muscle fatigue from excessive time spent on electronic devices, many eye doctors recommend the 20-20-10 rule, which allows the eye muscles to rest. Every 20 minutes, your child should take his eyes off the electronic screen and look at an object at least 20 feet away for at least 10 seconds. This healthy habit allows your child to take frequent breaks from his electronic device. Parents should set guidelines on the amount of time that they allow their children to spend on computers, cell phones, and electronic books/toys, because these activities do not promote physical activity, and could contribute to childhood obesity and eye problems.
If your child spends an excessive amount of time on electronic devices, he may exhibit signs of vision problems including squinting, frequent eye rubbing, red eyes, head turns, unusual postures, and complaints of blurred vision. If your child avoids using the computer, this may also be a sign. Your awareness of their visual difficulties will only be apparent if you watch and work with your child. To make sure that our children are ready for computer use at school, schedule a comprehensive eye examination with your optometrist at the start of every school year.
For More Information about Obesity and Vision Problems from Excessive Computer Use:
http://www.allaboutvision.com/
Guest Columnist: Janet Caputo, PT, DPT, OCS specializes in orthopedic and neurological rehabilitation. Dr. Caputo is clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC.
Read “Health & Exercise Forum” in the Scranton Times-Tribune every Monday. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com.
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Get the Most Out of Your New Knee: Part 2 of 2
Ted Schoch, PIAA football official from NEPA, has spent the past 9 months preparing for the high school football season with the same vigor and passion as a young athlete. You may have seen him biking through Dalton or running drills on the sports facilities at Abington Heights High School. He has been recovering from a total knee replacement and met his goal of returning to work as a football official in this year’s Dream Game. He learned that it takes much more than traditional home exercises to “get the most out of your knee replacement” and get back in the game!
Total knee replacement surgery is a very successful orthopedic surgery as more than 600,000 are performed in the United States each year. More than 95% of patients with TKR are satisfied with the outcome one year later according to the American Association of Orthopaedic Surgeons. Pain relief with daily activities was the most important factor for most patients. Those dissatisfied are often younger and tended to have a long history of an active lifestyle. Many of these patients may have unrealistic goals and expectations. It is recommended that these patients have better preoperative counseling and longer, more aggressive rehab to meet the goals of a more active lifestyle after surgery. The purpose of this column is to present a more advanced rehab program for “fine tuning” in order to make a full recovery for those hoping to hike, ski, play tennis, golf, etc. AND for those who seek better function in daily activities with their new knee.
Despite advances in knee joint implants (e.g. more durable materials, improved simulation of anatomical knee joint movement), some patients continue to report dissatisfaction with their post-operative function! Patients often complain about difficulty; entering or exiting a car, descending stairs, bending to the floor, and rising from a commode. All of these activities have one thing in common…they require the ability to perform a partial squat: controlled lowering of the body weight against gravity, not any easy task!
In order for a replaced knee to perform optimally, the hip and ankle must be challenged with exercises similar to the following:
In addition to adequate ankle/hip mobility and strength, the ability to differentiate between the hips and lower back (i.e. body awareness) requires proprioceptive training:







Get what you want out of your new knee and don’t settle for less!
MODEL: Vanessa Borgia
Guest Columnist: Janet Caputo, PT, DPT, OCS is clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC in downtown Scranton.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum" in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email:drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 1 of 2
Ted Schoch, PIAA football official from NEPA, has spent the past 9 months preparing for the high school football season with the same vigor and passion as a young athlete. You may have seen him biking through Dalton or running drills on the sports facilities at Abington Heights High School. He has been recovering from a total knee replacement and met his goal of returning to work as a football official in this year’s Dream Game. He is more excited than usual to officiate this football season. He, like many others, learned that it takes much more than traditional home exercises to “get the most out of your knee replacement” and get back in the game!
Total knee replacement surgery is a very successful orthopedic surgery as more than 600,000 are performed in the United States each year. More than 95% of patients with TKR are satisfied with the outcome one year later according to the American Association of Orthopaedic Surgeons. Pain relief with daily activities was the most important factor for most patients. Those dissatisfied are often younger and tended to have a long history of an active lifestyle. Many of these patients may have unrealistic goals and expectations. It is recommended that these patients have better preoperative counseling and longer, more aggressive rehab to meet the goals of a more active lifestyle after surgery. The purpose of this column is to present a more advanced rehab program for “fine tuning” in order to make a full recovery for those hoping to hike, ski, play tennis, golf, etc. AND for those who seek better function in daily activities with their new knee.
Despite advances in knee joint implants (e.g. more durable materials, improved simulation of anatomical knee joint movement), some patients continue to report dissatisfaction with their post-operative function! Patients often complain about difficulty; entering or exiting a car, descending stairs, bending to the floor, and rising from a commode. All of these activities have one thing in common…they require the ability to perform a partial squat: controlled lowering of the body weight against gravity, not any easy task! The partial squat maneuver requires not only adequate mobility and strength at the hip, knee, and ankle but also equal weight bearing on both legs. The more advanced activity of descending stairs in a step over step manner requires even more effort as the leg muscles and joints must be strong and mobile enough, to support the body’s weight independently!
Studies show that even after two months of rehabilitation following knee replacement surgery, patients continued to place more body weight over their non-operative limb! This problem occurs for several reasons: (1) Continuation of a habit of walking in a manner to avoid a knee pain before surgery (compensating to avoid pain from the arthritic knee), (2) Continuation of a the “learned” compensation following knee replacement (compensating to avoid knee pain from surgery), and (3) reflex muscle inhibition (when the body experiences pain, the muscles are inhibited to contract in order to avoid pain). If not corrected, these three behaviors, whether acquired, learned, or automatic, will continue for a long time following knee replacement surgery and prevent the best possible outcome for the individual.
In order to perform the functional squat maneuver necessary for the functional, daily activities individuals must possess adequate mobility at their hips, knees, and ankles.
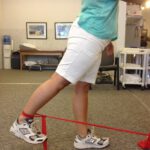
Functional Squat
Hips must bend > 90°, knees must bend at least to 90°, and ankles must bend to approximately 12° to 15°
Note: Ted Schoch, PIAA Football Official from NEPA demonstrates a functional squat with slight compensation in his right knee replacement due to lack of range of motion in right hip and ankle.
In addition to adequate leg joint flexibility, a proper squat requires strength of several key muscles: gluteus (buttocks), hamstrings (back of the thigh), quadriceps (front of the thigh), and the gastroc (calf).
During rehabilitation following knee replacement, even though knee function is paramount, failure to address hip/ankle mobility/strength may interfere with the restoration of important, daily tasks. In order for a replaced knee to perform optimally, the hip and ankle must be challenged with exercises similar to the following:
Calf Stretching
Calf Strengthening




MODELS: Ted Schoch; Vanessa Borgia
Next week read Part 2 for more advanced exercises to get the most out of your new knee…don’t settle for less
Guest Columnist: Janet Caputo, PT, DPT, OCS is clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC in downtown Scranton.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune Part 2 of 2 entitled, “Get The Most Out of Your New Knee.”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
