
Guest Author: Robin Tanner MD3, 3rd Year Medical Students at Geisinger Commonwealth School of Medicine (GCSOM)
Robin Tanner MD3 is a third year medical student at Geisinger Commonwealth School of Medicine. Originally from Danville, Pennsylvania, Robin received her bachelor’s degree from Auburn University in Auburn, Alabama. Aside from studying medicine, she enjoys learning about World War II, politics, classical literature and new languages. She volunteers with different pediatric organizations including the Make-A-Wish Foundation and Camp Victory. She hopes to pursue a career that incorporates medical education, pediatrics and global health.
It’s routine to be asked, while visiting a doctor’s office “what medications are you taking?” You give the doctor a list of medications and are ready for the next question at your visit. Wait, what about those vitamins you have been taking? He probably doesn’t need to know that right? They are gummies with smiley faces on them. Why would a doctor care if you eat a gummy every day? About 48% percent of adults take some sort of supplementation as a part of their daily routine. Vitamins show minimal significant benefits in healthy individuals and can even cause negative side effects when taken with specific medications.
Last week’s article discussed the purpose of vitamin supplementation and how it applies to the average healthy individual. Although it is not needed in individuals who eat a well-balanced diet, there are many people who can benefit from vitamins and people who should stay away from them.
Many diseases and conditions which benefit from vitamin supplementation are due to higher demands on the body, decreased levels in vitamin stores in the body or poor absorption from food. Depending on the disease or condition, a vitamin supplementation may provide symptomatic relief or prevent progression of the disease. On the other hand, some vitamins can react with specific medications to cause additive effects, counteract the medication’s effects, or even potentiate side effects. The following are some circumstances where vitamins may or may not be beneficial.
Women who are pregnant or are planning to become pregnant are strongly suggested to use prenatal vitamins. An important component of prenatal vitamins is folic acid (vitamin B9). In fetal development, the neural tube will grow to become the brain and spinal cord. Folic acid is important in helping to prevent neural tube defects such as anencephaly (a condition where the baby is born without major portions of the brain) and spina bifida (where a baby is born with an opening in the spinal cord exposing the nerves).
Children who are nursed should receive vitamin D supplements until weaned to whole milk containing vitamin D. Children who are nursed also benefit from iron supplementation until iron-containing foods (such as spinach, broccoli or meats) are introduced into the diet. For children who use formula, they typically reach their daily requirements due to supplementation in the formula itself.
Anemia occurs when there is a decrease in the amount of red blood cells circulating in the blood. Symptoms include fatigue, dizziness and shortness of breath. Anemia can be due to a deficiency of vitamin B12, folate (B9) or iron. These substances help red blood cells divide and function properly. When the body is lacking, there is a decrease in the amount of functioning red blood cells to carry oxygen to the body. A blood test at a doctor’s office can help determine the cause of the anemia and will lead to appropriate supplementation.
As women age, the levels of estrogen decrease in the body which leads to an increased in bone breakdown. This is a common complication in postmenopausal women and can lead to bone pain and fractures. Vitamin D and calcium supplementation can help improve bone health and decrease the risk of bone fractures in this population.
Certain digestive disease such as Chron disease or other inflammatory bowel diseases cause impairment in the absorption of some molecules. Supplementation with iron, B vitamins, vitamin D, zinc and magnesium could be beneficial to maintain the recommend daily intake.
Long term metformin use can lead to a B12 deficiency. Although B12 deficiency takes years to develop (due to large amounts stored in the body), the symptoms may be confused with diabetic neuropathy. B12 supplementation may prevent nerve damage due to the deficiency. Levels are commonly monitored in these patients for such a reason.
The retinoids are a class of drugs similar to vitamin A. A commonly prescribed retinoid is isotretinoin, commonly called Accutane, used in the treatment of acne. Increased levels of vitamin A from supplementation and drug administration can increase the risk of vitamin A toxicity which can lead to nausea, vomiting and vision changes.
Warfarin (Coumadin) is a commonly prescribed drug to decrease the risk of blood clot formation. Warfarin prevents clotting by inhibiting and enzyme which requires vitamin K to function. Using supplementation of vitamin K while using Warfarin to prevent clots can reverse the effects of Warfarin and thus increase the likelihood of developing blood clots.
Niacin (vitamin B3) can affect cholesterol levels, lowering LDL cholesterol (“bad cholesterol”) and increasing HDL cholesterol (“good cholesterol”). Statins are one of the most prescribed drugs in the United States. They decrease the amount of cholesterol made by the liver thus decreasing blood cholesterol levels. However, research has shown that when combining these two medications, there is no increased benefit. Niacin may even cause a small increase in risk for muscle pain and breakdown, a statin side effect.
Vitamin supplementation has the potential to be beneficial and harmful. Therefore, it is important to disclose to medical professionals all current medications along with any supplementation one may be taking. This is especially true when considering adding a new drug to daily regimens. If you have been diagnosed with a medical condition or are taking medications, it is important to talk to your medical provider before beginning over the counter supplementation. So yes, your doctor does want to know if you are eating a smiley face gummy every day.
Sources:
National Institutes of Health (NIH) - Office of Dietary Supplements (ODS) – Fact Sheet for Health Professionals
Blumberg, J., Frei, B., Fulgoni, V., Weaver, C., & Zeisel, S. (2017). Impact of frequency of multi-vitamin/multi-mineral supplement intake on nutritional adequacy and nutrient deficiencies in US adults. Nutrients, 9(8), 849.
Medical Reviewer: James W. Joseph, MD, Geisinger Family Practice, Elysburg, PA and GCSOM Family Medicine Practice Clerkship Director
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
Guest Author: Robin Tanner MD3
3rd Year Medical Students at Geisinger Commonwealth School of Medicine (GCSOM)
Robin Tanner MD3 is a third year medical student at Geisinger Commonwealth School of Medicine. Originally from Danville, Pennsylvania, Robin received her bachelor’s degree from Auburn University in Auburn, Alabama. Aside from studying medicine, she enjoys learning about World War II, politics, classical literature and new languages. She volunteers with different pediatric organizations including the Make-A-Wish Foundation and Camp Victory. She hopes to pursue a career that incorporates medical education, pediatrics and global health.
We have all seen that one aisle at the grocery store, pharmacy or health food store that overwhelms us …the aisle with hundreds of little bottles with tiny font and colorful pills. It’s the vitamin aisle. It is full of pills reaching from the floor to ceiling, all of which claim to improve your health in some aspect. Which do you pick? One says that it will improve your energy. Others claim to make your hair grow faster. Is this all too good to be true? This one aisle is just a small piece of a $30 billion industry in the United States. How did this happen? Is it money well-spent?
What is a vitamin? In a general sense, it is a substance which is used by the body for processes needed for growth and development. They assist in the building of proteins and the breakdown of products to create energy for a cell. Many vitamins are consumed in our everyday meals such as vitamin C, found in lemons, and vitamin A, found in carrots. Many studies have focused on the amount of each vitamin that is required to stay healthy. These studies have lead to a recommend daily intake of each vitamin in the diet, which can be found on the FDA’s website.
Scientists have studied vitamins for many years. In 1913, Thomas Osborne discovered vitamin A. In 1922, Edward Mellanby discovered vitamin D. Many of these discoveries where guided by research focusing on a specific disease where the underlying cause of disease was a lack of the specific vitamin. Many current scientists believe this may have led to the beginning of vitamin supplementation: to avoid the diseases caused by a deficiency.
All throughout the 1900’s vitamins were advertised to improve energy and job performance, as alternative to healthy food choices, and as a way to have more fun in general. Advertisements like these can lead to confusion regarding the purpose of vitamins and when to use them. Even today, vitamins are still advertised to increase energy and avoid unwanted illnesses.
So, do you need vitamin supplementation? Many research trials have failed to demonstrate a significant benefit from vitamin supplementation in preventing diseases which are not caused primarily from lack of a specific vitamin itself. This is especially true in individuals who eat a well-balanced diet, because many of the vitamins needed for the body to work properly are already present in the food we eat. Moreover, taking a vitamin supplement does not provide an alternative to a healthy diet.
Some research has shown that there is even a potential for harm when ingesting a vitamin level higher than the recommend intake. For example, Vitamin E and folic acid may lead to increased risk hemorrhagic shock, a condition where bodily organs do not receive enough blood and oxygen. Vitamin supplementation also has a potential risk for harm when mixed with certain medications. Therefore, it is important to tell a medical provider all medications along with supplementations one is taking.
Although tempting, vitamin supplementation may not be the most beneficial method for achieving good health. Maintaining a healthy diet and participating in regular exercise is the most important step to living a healthier life and to help in the prevention disease. Although vitamin supplementation is nonessential for most, there are specific individuals and diseases which may benefit from vitamins. Please read next week’s article to review those who can benefit and those who can be harmed from vitamin supplements.
National Institutes of Health (NIH) - Office of Dietary Supplements (ODS) – Fact Sheet for Health Professionals
Blumberg, J., Frei, B., Fulgoni, V., Weaver, C., & Zeisel, S. (2017). Impact of frequency of multi-vitamin/multi-mineral supplement intake on nutritional adequacy and nutrient deficiencies in US adults. Nutrients, 9(8), 849.
Medical Reviewer: James W. Joseph, MD, Geisinger Family Practice, Elysburg, PA and GCSOM Family Medicine Practice Clerkship Director
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week: The Truth About Vitamins Part II of II
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
Like many in NEPA, I enjoy winter in great part due to my love for downhill and cross-country skiing. However, with age and wisdom, I have become much more aware of the need for safety through the use of proper equipment, good technique and preseason conditioning. Every November 1st I begin my preseason ski conditioning program and while watching my routine, a local ski enthusiast and patient asked me if I would offer some tips for preseason conditioning for skiing. The following is an updated version of the program.
The following exercises will target the essential stability, agility, and eccentric training requirements for the prevention of skiing injuries. A BosuR Ball is a useful tool to challenge your balance and strength for skiing and other sports. It is flat on the bottom and round on the top. (www.bosu.com $70 - $110.) However, standing on one or two pillows can work.
Traditional exercise such as weight training for quads, hams, gluts etc are valuable. Also, elliptical and stepper equipment and exercise bikes are important. However, the following exercises are specific to the needs of the downhill and cross-country skier.
Monster Walk Out & In (PHOTOS 1A, 1B)
Ski BosuR Squat (PHOTO 2)
Ski BosuR Step Down (PHOTO 3)
Ski Pole Lunge (PHOTO 4)





Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is an associate professor of clinical medicine at GCSOM.
Part 2 of 2

November is National Chronic Obstructive Pulmonary Disease (COPD) month. COPD is the fourth leading cause of death in the United States, according to the Centers for Disease Control and Prevention. This problem refers to a group of lung diseases that causes damage to the airways and air sacs in the lungs. People with COPD suffer from diminished airflow and difficulty breathing. Emphysema and chronic bronchitis are two of the most common types of COPD. The damage can't be reversed, so treatment includes medications and lifestyle changes designed to control symptoms and minimize further damage, according to the Mayo Clinic.
Exercise is an important part of life for those with COPD because it improves the overall strength and endurance of respiratory muscles. When you exercise, muscles adapt and use oxygen more efficiently so your lungs don't have to work so hard. Also, in addition to improvement in breathing, exercise boosts mental health, helps maintain a healthy weight and blood pressure, and improves circulation. Most importantly, exercise will improve your quality of life with COPD.
Before you begin an exercise program, see your family physician or pulmonologist for approval. Then, see a physical therapist to design a program specific for your needs. Always begin slowly and rest if you get short of breath, have chest pain, feel dizzy or sick to your stomach.
While not all of these endurance exercises may be appropriate for you, one or two of these may offer a good starting point.
A. Walk Around the House: Start walking around the house for 1-2 minutes nonstop. Every 1-2 hours. Then, add 1-2 minutes every week.
B. Static Marching: hold onto the countertop or back of chair and march in place for 30 seconds. Rest 1-2 minutes and repeat. Do 5 cycles. Add 5-10 seconds every week.
C. Climb the Steps: If you can do so safely, use the steps for exercise 1-2 times per day. Then, add 1-2 times per day.
D. Walk the Mall/Treadmill: If you are able to get out of the house and can tolerate more extensive endurance exercises, get out and walk the malls or use a treadmill.
E. Recumbent Bike: If balance is a problem, but you can tolerate more extensive endurance exercise, use a recumbent bike (a bike with a backrest)
Walking is free exercise and can be done in some form by almost everyone…even with an assistive device such as a cane or walker. For those with COPD who are active and fit – walk 4-5 days per week for 30 to 45 minutes. Less fit individuals can walk for 15 to 20 minutes. For those with COPD who are in poor condition and have significant SOB – walk for 2-3 minutes (to the bathroom or around the house) every 30 to 45 minutes. Try not to sit for 60 minutes without getting up and walking around.
Posture exercises are designed to keep your body more upright and prevent rounded shoulders and forward head/neck. More erect posture promotes better breathing.
A. Row-The-Boat - Pinch shoulder blades together as if you are rowing a boat.
B. I-Don’t-Know – Shrug shoulders up toward the ears as you do when you say “I don’t know.”
C. Chin Tucks – Bring your head back over your shoulders and tuck your chin in
A. Bicep Curls – sit in chair and bend your elbows up and down with a can of peas in your hands
B. Wrist Curls – as above but bend your wrists up and down
C. Chair Push-ups – Push up with your arms to get out of a chair
D. Saw Wood – pull a light resistance band (yellow) back from a door knob as if you were sawing wood.
A. Hip Hikes – Sit in chair and march by hiking your hip and lifting up your heel 4-6 inches off the floor
B. Leg Kicks – Sit in chair and kick your knee out straight – then bend it down to the floor
C. Hips Out and In – Sit in chair and bring your knees in and out against a resistance band
D. Toe Raise/Heel Raise – Sit in chair and raise your toes up – then raise your heels up
A. Diaphragmatic Breathing - The diaphragm muscle is essential for breathing. While sitting or lying down, put one hand on your abdomen and the other on your chest. Slowly inhale through your nose and try to separate the hand your stomach from the hand on your chest. Then, slowly exhale through pursed lips.
B. Pursed Lipped Breathing - breathe in through your nose slowly for 3- 5 seconds. Then, purse your lips as though you're going to whistle. Lastly, exhale slowing through the pursed lips over 5 to 10 seconds.
More Information: “Better Breathers Club,” in conjunction with the American Lung Association, offers a free local support group to help patients and their families suffering from COPD and chronic lung disease. www.lung.org
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton, PA and is an associate professor of clinical medicine at GCSOM.
LUNG DISEASE
Part 1 of 2
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
GCSOM GUEST AUTHOR: Nicholas Czelatka, MD1
Nicholas is a currently a first-year medical student Geisinger Commonwealth School of Medicine. He is a graduate of Stony Brook University and Islip High School. Nicholas grew up in Long Island and enjoys the outdoors with activities ranging from golfing to surfing to skiing.
Chronic obstructive pulmonary disease (COPD) has become the fourth leading cause of death and is one of the only major chronic diseases which have seen an increase in mortality rates. COPD includes emphysema, chronic bronchitis and asthma.
Patients with COPD suffer from progressive shortness of breath, cough, wheeze, and sputum production. Most patients with emphysema have been cigarette smokers.
Patients with emphysema develop obstruction to airflow as a result of narrowing of bronchial tubes due to excess mucous, smooth muscle constriction, and destruction of lung tissue. Eventually, the lungs become over distended, which leads to overexpansion of the chest itself. This process leads to the so-called ''barrel chest'' appearance of patients with advanced COPD.
The most common symptom of COPD is shortness of breath. Initially, the patient complains of shortness of breath only with exertion, but symptoms progress over time to include difficulty breathing, even at rest. Eventually the disease worsens to the point that oxygen is required and the patient may become severely disabled.
Treatment of COPD starts with smoking cessation, and, when symptomatic, patients are started on inhaled bronchodilator medications. Some of these medications include albuterol, ipratropium, titotropium, and inhaled steroids. Long-acting bronchodilators such as formoterol or salmeterol and theophylline medications may be added. Oxygen is added when the patient's own oxygen level falls to a certain point. In fact, oxygen is the only therapy that has been shown to prolong the life of patients with COPD.
Over time, patients with COPD decrease their level of activity due to the sensation of shortness of breath. This downhill slide eventually leads to a very sedentary existence. Recent studies have shown that COPD not only affects the lungs, but is a condition which affects the diaphragm and the peripheral muscles. Patients with COPD have been shown to have abnormal limb muscles as a result of deconditioning and systemic inflammation. Exercise is the best treatment to delay or prevent deconditioning.
Studies have shown that several factors can actually worsen the symptoms associated with COPD. For example, stress can negatively impact breathing patterns and lead to anxiety which worsens shortness of breath. The weather can also aggravate symptoms, such as season climate and high humidity changes. Irritants, like smoke (first or second hand), as well as cooking smoke, cleaning aerosols and perfumes should be avoided. Overexertion, not to be confused with a necessary and appropriate exercise program, can lead to shortness of breath and other symptoms. Noncompliance, such as not using oxygen, taking medications and performing a home exercise program as directed, will aggravate symptoms.
Pulmonary rehabilitation has been shown in numerous studies to decrease the shortness of breath associated with COPD. Exercises to strengthen the arms are helpful to assist patients in performing activities of daily living such as combing hair, cooking, and reaching objects above their heads. Walking and riding a stationary bike are helpful to exercise the leg muscles, especially the large thigh muscles. Despite the fact that exercise programs may not improve lung function, the patients overall level of function are almost always improved. It is recommended that a pulmonologist and physical therapist should be consulted to establish an appropriate and individualized exercise program (to be discussed in next week’s column on COPD).
Sources: www.cdc.gov
Medical Reviewer: Dr. Gregory Cali, DO – is a pulmonologist (lung doctor) in Dunmore, PA.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” COPD Part 2 – Exercise with COPD.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton, PA and is an associate professor of clinical medicine GCSOM.
Part 3 of 3
GUEST COLUMNIST: Paul Mackarey, Jr. DPT
Lower back pain (LBP) is one of the most common problems in our society as well over 85-90% of all Americans will suffer from it at least once in their lives. It affects productivity in the workplace and lifestyles at home. The medical costs of treatment including; medication, physical therapy, alternative medicine, and surgery are staggering. It is generally agreed that prevention is the best treatment for LBP.
TOP TIPS FOR THE PREVENTION OF LOWER BACK PAIN


GUEST COLUMNIST: Paul Mackarey, Jr. DPT is clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC where he specializes in the prevention and treatment of neck and LBP.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at GCSOM.
Visit your doctor regularly and listen to your body.
Part 2 of 3
GUEST COLUMNIST: Paul Mackarey, Jr. DPT
Lower back pain (LBP) is one of the most common problems in our society. In fact, over 85-90% of all Americans will suffer from back pain at least once in their lives. It affects productivity in the workplace and lifestyles at home. The medical costs of treatment including; medication, physical therapy, alternative medicine, and surgery are staggering. It is generally agreed that prevention is the best treatment for LBP.
Last week, we discussed the importance of early intervention, controlled movement and proper exercise as a very important part of minimizing the lasting effects felt from a new or recurring exacerbation of back pain. However, it is important to have an understanding of what is the “best” type of movement and exercise for your back. This differs from person to person. Often your spine has a “directional preference” or a specific direction that fosters the healing process. Moreover, this preference will also limit movement in the wrong direction which may delay healing. The two most common and easily assessed directional preferences are flexion directional preference (FDP) or bending forward and extension directional preference (EDP) or bending backward.
Flexion Directional Preference: FDP occurs in people with back pain who experience little to no pain when bending forward or sitting down. Due to the fact that the back undergoes normal and natural changes as we age, the position we are most comfortable in also changes. Typically, this change occurs around the age of 50 – 60 years old; however, it can begin earlier depending on the individual. If you find that sitting or bending forward is a position of comfort and eases your back pain than you have FDP and your back can heal faster when selecting exercises that focus on repeated bending. Exercises such as single knee to chest, double knee to chest or child pose may be the best for you. (See Photos 1-3 below)
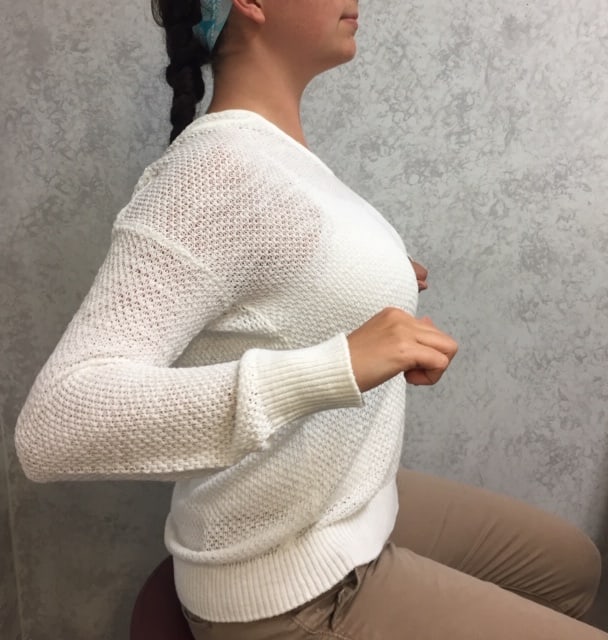
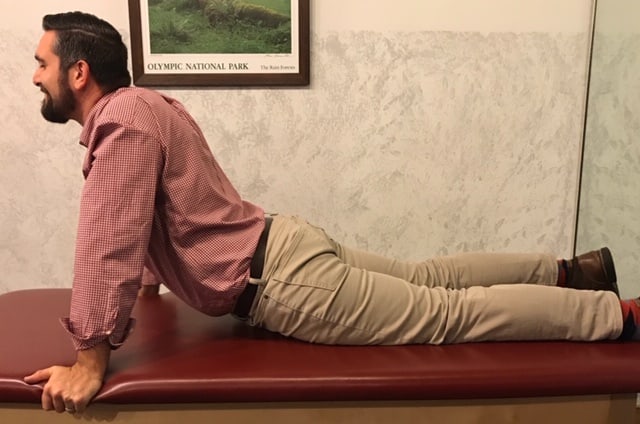
Extension Directional Preference: EDP occurs in people with back pain who experience little to no pain when standing, walking and/or bending backwards at the hips. This is best assessed when lying prone (on your belly) and bending backwards by propping up on your elbows/forearms. If this position is pain free than you may have EDP. Commonly, individuals that fall in this category range from the age of 45 years old and younger. Exercises that focus on the direction of extension are best. Selecting exercises such as prone on elbows, prone press up, open books and modified planks are best. (See Photos 4-7 below)
Always consult with your physician or physical therapist before beginning a new exercise program. Please perform slowly, hold for 3-5 seconds and repeat 6 times each 6 times per day. Do not continue the exercises if symptoms worsen.
PHOTO 1: Single Knee to Chest (best for FDP) While lying on your back grab the back of the one knee and pull the knee toward your chest. Alternate knees.
PHOTO 2: Double Knee to Chest (best for FDP) While lying on your back grab the back of the both knees and pull knees toward your chest
PHOTO 3: Child’s Pose (best for FDP) Begin in quadruped position (on hands and knees) and bend at the hips as your butt moves toward your heels.
PHOTO 4: Prone on Elbows: (best for EDP) While lying on your belly, prop up on your forearms to extend your lower back.
PHOTO 5: Prone Press Up: (best for EDP) While lying on your belly, prop up on your forearms, then straighten your elbows to further extend your lower back.
PHOTO 6: Open Book: (best for EDP) While lying on your side with the bottom knee straight and top knee bent, rotate by opening the arms and reaching behind you. Relax the back and let gravity give you the stretch. Then, alternate sides.





GUEST COLUMNIST: Paul Mackarey, Jr. DPT is the clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC where he specializes in the prevention and treatment of neck and LBP.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week – LBP Part 3 of 3
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at GCSOM.Visit your physician regularly and listen to your body
…THE MORE YOU KNOW
Part 1 of 3
GUEST COLUMNIST: Paul Mackarey, Jr. DPT
One of the most common problems people come to our office with is lower back pain (LBP). Studies show that 80-90% of adults in the USA will experience lower back pain at one or more times in their lives. It is the second most reported reason for work absences and is so common that one might even describe it as “normal.” The good news is that 80 percent of those with LBP get better within three months! However, it is important to know “the truth about lower back pain” to ensure that you do NOT become one of the twenty percent! For example, when treatment is delayed and/or mismanaged, the problem may become chronic. In fact, LBP is a commonly associated with opioid abuse.
Management of LBP has become a financial burden as 86 billion dollars (25% of healthcare costs) are spent on the problem each year. It is the equivalent of the money spent on cancer treatment and much of it is spent on unnecessary tests and ineffective treatment. The purpose of this column will be to address the myths associated with LBP and educate consumers in order to make more informed decisions related to this problem.
There are two types of LBP, acute and chronic. Acute LBP is back pain that has devlpoed recently (within the last 3 months). Acute LBP is the leading cause of disability in the US among individuals younger than 45 years old. Chronic LBP is associated with pain that lasts more than three months. Traditional treatments include: nonsteroidal anti-inflammatory drugs, opioids, injections, manipulation and physical therapy, massage therapy, and, when all else fails, surgery. While many of these treatments can help, the efficacy of one approach over another is limited. However, what is clear, according to current research, is that early intervention is critically important to promote early healing, prevent further damage and limit the likelihood that the problem will become chronic.
The spine consists of 24 moving vertebrae, a fused sacrum and tailbone, and shock absorbing discs between each moving segment. The spine is designed to provide support and protect the spinal cord while remaining flexible for movement and function. Spinal nerves exit the spinal cord at each segment to deliver messages from your brain to your extremities. Pressure on one of these nerves can cause pain, numbness, tingling, or weakness. Muscles can also become weak and imbalanced and lead to wear and tear on the spine.
LBP can occur from many causes. Some of these include: muscle strain, disc degeneration, arthritis, scoliosis or curvature of the spine, instability from trauma or degeneration, acute trauma from a motor vehicle accident account or a fall. Many workers are also at high risk for lower back pain. But remember, regardless of the cause, 80% of those with LBP will get better within 3 months…if managed properly. And, the best treatment for LBP is prevention, which will be discussed in LBP-Part II.
MYTH 1: I need to get an MRI before I begin my treatment for LBP.
NOT TRUE. You may know someone who has been told that they have to receive 6 weeks of physical therapy before their insurance will approve an MRI. This is for good reason. First, the insurance company knows that recent research shows that most people with LBP will be better in 6 weeks with proper management, like physical therapy. Second, it is also well-known in the medical community, that 30% of all MRI’s find problems in the spine in people without LBP (false positive). MRI’s are necessary when certain “red flags” are present such as: pain below the knee associated with weakness in the leg, history of cancer, recent trauma and others.
MYTH 2: I need to see a spine surgeon before I can begin treatment for LBP.
NOT TRUE. While spine surgeons (orthopedic or neurosurgeon) are critically important in some cases of LBP, they are rarely seen as a first visit. However, this is not a reason to delay treatment because time is of the essence. Current research associates better outcomes with early intervention. So, advocate for yourself and notify or visit your primary care physician to ask about early conservative treatments such as physical therapy.
MYTH 3: When I get LBP I need pain medication.
NOT TRUE. You cannot read a newspaper today without finding an article about the opioid crisis in our country. Over prescription of opioids has contributed to this problem and LBP was the number one reason only a few years ago. The US, representing only 5% of the world’s population, consumes 99% of global hydrocodone use. As a result, in 2016, the CDC recommends ‘non-drug approaches” to LBP management such as physical therapy, acupuncture, massage and others.
MYTH 4: If I have LBP I should stop moving: bending, walking, and exercising to prevent further damage.
NOT TRUE/TRUE. While it is important to limit certain movements and exercises that may contribute or worsen the problem, avoid all movement and activity may, in fact, contribute to the problem. For example, lifting heavy objects from the floor, sitting too long, running, jumping, performing sit ups, toe touches etc. should be avoided in the early stages of recovery. However, movement in relatively pain free positions is encouraged. For example, slow walking (10-15 minutes) intermittently throughout the day (2-3 times) is better than sitting all day. If you sit at work most of the day, it is advisable to alternate between sitting (20-30 minutes) and standing (10-15 minutes) at a standing desk. Avoiding a vigorous exercise routine is advisable until you consult with your physical therapist or physician.
MYTH 5: If I still have LBP in 6 months, than I need to have surgery.
NOT TRUE. Just because you have LBP does not mean you require surgery, even if it lasts for 6 months. Surgery is rarely performed for LBP alone and is usually limited to those with pain below the knee associated with weakness and for those with other neurologic signs. Remember, we all heal and recover at differently and while most recover from LBP in 3 months, others may require 9 – 12 months. Be sure you exhaust all conservative options and seek reputable medical advice: primary care physician, physical therapist (specializing in spine), physiatrist, and spine surgeon.
GUEST COLUMNIST: Paul Mackarey, Jr. DPT is clinic director at Mackarey & Mackarey Physical Therapy Consultants, LLC where he specializes in the prevention and treatment of neck and LBP.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week – LBP Part 2 of 3
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at GCSOM.Visit your doctor regularly and listen to your body.
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
Guest author: Branston Allen
Branson is a currently a 4th year medical student at the Geisinger Commonwealth School of Medicine. He is a graduate of Lock Haven University and Shippensburg Area High School. Branson grew up in Shippensburg as an avid outdoorsman and enjoys activities ranging from hunting to fishing to camping.
As the temperature drops and the leaves fall, nearly one million Pennsylvanians take up their trusty deer rifles and plunge into the woods with hopes of dragging out a prized white-tailed deer. Historically, rifle season commences on the first Monday after Thanksgiving, however, this year, for the first time it will begin the Saturday after Thanksgiving and archery season has been active since October 5th. Hunters and loved ones often worry about potentially fatal misfortunates that can occur while secluded in the forest. These concerns range from stray bullets to tree stand falls. However, according to many experts, a heart attack is up to three times more likely to claim a hunter’s life than an errant bullet or arrow.
One Man’s Story
As a third year medical student, I’ve actually already encountered a local gentleman whose heart carries the scar of a heart attack he experienced while hunting. To protect his identity, I’ll refer to him as John. John – “November was always my favorite month of the year. Thanksgiving is a nice holiday and it’s great to see family. But the best part about it is deer season”. John is a 68 year old, recent retiree who was born and raised in Luzerne County. Like a lot of NEPA residents, he probably eats a few too many pierogis and drinks a few too many beers, but otherwise is pretty healthy. He worked most of his life in a local warehouse, and always requested off for the first 3 days of deer season. Last deer season was almost John’s last. “It was the second day of the season and I finally managed to get a clean shot at a nice sized doe. I was dragging her out whenever I got this massive pain across my chest. I was sweating like crazy and it felt like an elephant was sitting on my chest. After I few minutes, I got really nervous and called my wife. She told me to call 911” – John. Fortunately for John, his story had a happy ending. “The doc told me I had about a 99% block of a vessel in my heart that is called ‘the widow-maker’ and that I experienced a mild heart attack. Thankfully, they were able to fix me up with surgery, and I feel like lucky to still be here today”.
Risk Factors
Most people know a man like John and these are the type of people who we worry most about having heart attacks while they are hunting. The American Heart Association has identified men over the age of 45 and females above the age of 55 as the population most likely to suffer from cardiovascular disease. According to the Pennsylvania Game Commission, the majority of hunters are males of the age of 45, and these individuals are often overweight and don’t get much exercise throughout the year. When deer season comes, they’re putting strain on their muscles and heart in a way that their body isn’t used to dealing with. This increased demand on their hearts causes their heart rates to soar and can produce some of the tell-tale signs of heart disease. These include chest pain, arm pain or numbness, and shortness of breath. Additional risk factors such as high blood pressure, high cholesterol, obesity, and a sedentary lifestyle also increase one’s chances of suffering a heart attack.
What makes hunting especially scary is it stresses your body in ways everyday life doesn’t. Hunters must contend with the elements and temperatures associated with late November in Pennsylvania, the adrenaline surges associated with spotting a deer, and the daunting physical task of dragging 120+ pound deer out of woods if they shoot true. Any of these situations individually is capable of sending heart rates soaring. Complicating the hike into the woods on uneven terrain is the added weight of a gun, ammunition and other supplies. Also, trekking through mud or snow increases the physical demands exponentially. A research study out of Beaumont Hospital in Michigan found that the majority of hunters experience circumstances in which their heart rates exceed 85% of their maximum heart for sustained periods of time, which greatly increases the risk of a sedentary, unfit individual of sustaining a heart attack. Furthermore, hunters were more likely to demonstrate heart ischemia and arrhythmias during hunting than they were during a usual stress test with a treadmill. Arrhythmias are usually the cause of death when somebody experiences a heart attack, which makes these findings especially troublesome.
Prevention
So what can you do to keep yourself or your loved one safe during hunting season? First and foremost, if you experience any chest pain or shortness of breath on exertion, see your doctor immediately. Secondly, if you are a man over the age of 45 and have risk factors for heart disease such as hypertension, high cholesterol, diabetes, obesity, and/or live a sedentary lifestyle, talk to your doctor before you head out into the woods this year to make sure your heart can take all of the stress associated with hunting. Make sure that somebody knows where you’re at and can call for help if they don’t hear from you. If you have trouble walking or have risk factors for a heart attack, carry a cell phone with you and try to hunt near a place with vehicle access. Finally, just be smart and exercise caution while hunting. Listen to your body. Take as many breaks as you need while you are hiking into or out of your favorite hunting spot. If you manage to harvest a deer, take your time dragging it out of the woods. Drag, rest, and drag again. Better yet, call in backup and get some help with the drag, especially if you are a more seasoned hunter. You have earned the right to relax and employ the help of younger hunters to assist you. By doing this, you can ensure that this year’s deer won’t be your last.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
Recently, a young woman came to my office with complaints of severe middle and lower back pain. On her first visit, I carried her purse (big bag), to the treatment room to assess its weight. Then, I asked her permission to weight the bag and discovered that it weighed 8 pounds. While 8 pounds does not seem excessive, the woman weighed 120 pounds and, based on the research, would be advised to carry a 2.5 to 3.5 pound bag, (2-3% of her body weight).
A recent study shows that the average weight of a woman’s purse has increased by 38% and now exceeds 6 pounds. In spite of technological advances, women have not found a way to simplify their lives, or at least what they think they need in their lives. High tech gadgets have only added weight to a purse already filled to the brim.
On a whim, I decided to ask permission to examine the contents of some of my patient’s purses. A typical purse includes the following: hairbrush, cosmetic bag, mirror, feminine products, keys, and sunglasses, reading glasses, checkbook, wallet, coupons, water bottle, and medications. Additionally, I discovered heavy high tech products such as cellular phones, MP3 players, digital cameras, Bluetooth earpieces, and rechargers. Lastly, some women add the weight of a book or Kindle to the bag. Studies also show that the larger the bag and stronger the straps, the more items are stuffed in, resulting in a very heavy purse.
It is a pervasive attitude that a woman should never be stranded without her purse full of essentials. So, where is the problem? The problem is that carrying a heavy bag, usually on one side of the body, forces the body to tilt forward and in the opposite direction to compensate. Overtime, this change in posture leads to neck, middle and lower back pain.
SIGNS THAT YOUR PURSE IS TOO HEAVY:
Consider the following suggestions to promote healthy use of a purse and prevent injury.
SUGGESTIONS TO PREVENT INJURY:
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
