
Dr. William Iobst
Preventive Medicine -Create “Blue Zones” in NEPA
Guest CoAuthor: William F. Iobst, M.D., FACP is vice president for academic and clinical affairs and vice dean at The Commonwealth Medical College. He is a national leader in competency-based medical education and assessment of trainee performance. Prior to joining TCMC, Dr. Iobst served as vice president for academic affairs at the American Board of Internal Medicine (ABIM).
The media is captivated by the idea that a small, remote population – be it in the Himalayas or by the Mediterranean Sea – has discovered the secret to a long, healthy life. In these pages just last year you may recall Dr. Mackarey talking about “blue zones,” five specific locations on the planet where people enjoy life well past age 90. It’s intriguing to believe that an exotic locale or rare tropical fruits hold the magic charm to longevity. The reality is less magical. The truth is long-lived communities observe particular patterns of behavior and consistently make healthy choices we can all learn from and adopt.
We can think of these patterns of behavior as a form of medicine and the best form: preventive medicine. At The Commonwealth Medical College (TCMC), we are devoted to educating physicians of the future who recognize that medicine’s focus should include a focus on wellness. Moreover, our community emphasis at TCMC means we are deeply concerned with population health, which means we identify and work to change the unhealthy tendencies of the northeastern Pennsylvania population as a whole, tendencies that result in our having high rates of everything from cardiovascular disease to cancer to suicide. Let’s looks at how individuals can benefit from the preventive/wellness habits of blue zones AND how population health measures can be applied to benefit everyone.
When we think of our local population and compare it to the habits of the long-lived “blue zones,” what do we see? We see people who follow all the healthy rules many of us know but few of us follow: maintain a healthy weight, exercise, reduce your stress. In NEPA, many of us fall short of those wellness goals and we blame ourselves for lacking willpower or discipline. While it is certainly true that individuals should strive daily to make healthy decisions, when we look at the entire population, it’s obvious that there are very real differences between the population habits of NEPA and “blue zone” habits.
Let’s look at NEPA through the lens of population health and compare it to “blue zones.” As Dr. Mackarey wrote in 2015, below are some of the healthy behaviors associated with long-lived populations. As we discuss these behaviors through the lens of population health and wellness, it’s important to remember that individuals should always try to make wise decisions. Talking about barriers to wellness is a way for us to become aware of our unique challenges. We should not allow them to prevent us from achieving and preserving good health.
We can all learn from “blue zone” behavior and can individually commit to wellness and making the changes necessary to preserve it. However, as a community, we should also recognize that wellness isn’t solely the province of medicine. Every sector of community – from schools to law enforcement to government – can play a part. If we all work together, wellness and prevention are possible.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquiries related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

It happens every spring. A young pitching ace that started strong is now beginning to lose some speed on his fast ball. A third baseman that had no problems last week can’t throw to first base without pain. Shoulder pain in young baseball players occurs every spring just as the first robin, warmer temperatures, and the emerging sprouts of the spring flowers. And, the well-intended father/coach develops severe shoulder pain from hours of throwing balls at batting practice. The cause of the condition was the usual: not properly preparing the arm for the season.
Spring shoulder pain may be prevented with the proper preparation for the season. Throwing a baseball requires the shoulder to be very strong. In the off season, a shoulder can lose much of its essential strength. This loss will result in a deconditioned shoulder at the start of the first spring practice. Practicing with a deconditioned shoulder commonly results in sprain, strain and pain.
To avoid spring shoulder pain it is necessary to maintain shoulder strength. Strengthening exercises need to concentrate on three groups of muscles: the large power muscles of the shoulder, the muscles which stabilize the shoulder and the all important rotator cuff muscles. Strengthening power muscles of the shoulder is fairly easy. Pushups, lat pulldowns, bench presses, and bicep curls will cover all bases. While these exercises are important in maintaining strength and power of the throwing shoulder, they are not as important as the exercises for shoulder stabilizers and rotator cuff muscles.
The shoulder stabilizer muscles connect the arm to the torso. They serve as the foundation of the arm helping to stabilize the arm to the torso. The many stabilizing muscles include the trapezius and the rhomboid muscles. Exercise for theses muscles include: shrugs, T’s and Y’s. (See Photos A, B, C)
PHOTO A: SHRUGS: Stand with Dumbbell Weight in Hands, Raise Shoulders, Hold 3 Seconds and Repeat 10 times.
PHOTO B: “T’s”: Lying Face Down with Forehead on Towel Roll and With Light Dumbbell Weight in Hands, Raise Arms up in the shape of a “T.”
PHOTO C: “Y’s”: ”: Lying Face Down with Forehead on Towel Roll and With Light Dumbbell Weight in Hands, Raise Arms up in the shape of a “Y.”





The rotator cuff muscles have many functions. They are essential for the stability and proper function of the shoulder joint and in the throwing athlete they serve as brakes during the follow-through phase of a pitch. Exercises for the rotator cuff muscles include internal and external rotations. (See Photos D, E)
PHOTO D: Shoulder Internal Rotation: Stand with Exercise Band in the Throwing Hand and Elbow at the Side and Bent at 90 degrees, “Turn In - Against the Band.”
PHOTO E: Shoulder External Rotation: Stand with Exercise Band in the Throwing Hand and Elbow at the Side and Bent at 90 degrees, “Turn Out - Against the Band.”
While exercise is essential for conditioning the shoulder in the off-season, a graduated throwing program is also important. In the book The Athlete’s Shoulder, a throwing program is suggested. Training is every other day with a day’s rest in between. A ten minute warmup such as light jogging is suggested before throwing.
Day 1: 45ft – 25 throws - rest - repeat
Day 3: 45ft – 25 throws - rest – repeat – rest – repeat
Day 5: 65ft – 25 throws - rest - repeat
Day 7: 65ft – 25 throws - rest – repeat – rest – repeat
Day 9: 90ft – 25 throws - rest - repeat
Day 11: 90ft – 25 throws - rest – repeat – rest – repeat
Day 13: 120ft – 25 throws - rest - repeat
Day 15: 120ft – 25 throws - rest – repeat – rest – repeat
Day 17: 150ft – 25 throws - rest - repeat
Day 19: 150ft – 25 throws - rest – repeat – rest – repeat
Day 21: 65ft – 25 throws - rest - repeat
Day 23: 65ft – 25 throws - rest – repeat – rest – repeat
With the proper preparation, spring shoulder pain can be avoided in any baseball player.
Contributions: Gary E. Mattingly, PT, PhD is a professor at the University of Scranton, Dept of Physical Therapy
Models: Ron Chiavacci,, former professional baseball pitcher; Maggie Reilly, physical therapy student.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune

Stephanie Veit
Guest Columnist: Stephanie Veit. Stephanie is from Chesterfield, Missouri and will graduate with her MD degree from The Commonwealth Medical College in May 2016. She will begin her OB/GYN residency in July at Aurora Health Care in Milwaukee. Stephanie is dedicated to promoting women’s health and awareness.
Cervical cancer was once one of the leading causes of death in woman until the regular use of Pap smears became widespread practice according to the National Institutes of Health. The majority of cervical cancers are caused by high risk strains of sexually transmitted human papillomavirus (HPV). As a result, HPV testing has become part of the guidelines set out by The American College of Obstetricians and Gynecologists (ACOG) in screening for cervical cancer.
While several strains exist, HPV16 and HPV18 are the two strains of virus which cause the majority of all cervical cancers. The development of cervical cancer is step-wise in fashion and so pre-cancerous changes can be observed with Pap smears and further cervical changes can be predicted.
Women who have infections with high risk HPV strains have greater risk of developing pre-cancerous and cancerous lesions than those who do not have HPV infections. Guidelines now include testing for these high risk HPV strains as well as looking at the cells under the microscope with a Pap smear. The results of these two tests guide healthcare providers in the management of patients. Those women who test positive for high risk strains of HPV can go on to have more testing to see if they have any concerning lesions that could be pre-cancerous or cancerous. Women who are negative for the high risk strains but still test positive for HPV can be retested the following year to see if the infection has resolved.
Not every HPV infection leads to cervical cancer. In fact, many HPV infections are cleared spontaneously by the immune system, especially in younger women. 71% of women who were HPV positive but had normal Pap smears, tested negative for that specific HPV type at the following visit. The HPV infections which persist carry the increased risk of developing cervical cancer. Women who test positive for HPV at one visit and retest positive for HPV at a follow-up visit are at greater risk for precancerous and cancerous lesions then women who retested negative at a follow-up visit. Women who test positive for the same high risk strain of HPV at two visits in a row are at even greater risk, according to the National Cancer Institute. With this in mind, ACOG recommends repeat co-testing in one year if co-testing shows a negative Pap smear and positive HPV unless the patient tests positive for a high risk strain of HPV, thus allowing women time to clear the HPV infection spontaneously while also retaining the ability to treat those women who test HPV positive on repeat co-testing.
HPV testing is a good screening test on its own when compared to Pap smears alone. However, combining the two tests gives even better results. Women who test positive with co-testing consisting of both HPV testing and a Pap smear are more likely to have a true positive result. This allows for more women who have changes in their cervix to be identified and then treated. For example, if a woman tests negative for HPV, but has a borderline abnormal Pap smear, it is recommended that she receive repeat co-testing in three years. Should she test positive for HPV, especially a high risk type, and have an abnormal Pap smear, it is recommended that she receive a colposcopy (instrument assisted examination of the cervix) which allows healthcare providers to further visualize the cervix to determine if there is a lesion requiring further testing.
In summary, guidelines have been recommended for the screening of cervical cancer and management when screening comes back positive. Women who have not been infected with HPV have a very small chance of developing cervical cancer. One way to reduce the risk of being infected with HPV in the first place is with the HPV vaccine. The first HPV vaccine was introduced for use in 2006 and protects women against the most common strains causing genital warts and cervical cancer. The vaccine is targeted to girls and boys aged 11-12, and catch-up is offered to women up to age 26. Research shows that vaccinated women had a decrease of 88% in infection by HPV strains covered by the vaccine with a predicted 82% effectiveness of one dose of the vaccine. This essentially means that the vaccine is effective in preventing HPV infection and thus cervical cancer.
Cervical cancer has a yearly incidence for women under the age of 25 of 1.4 per 100,000 women. This number has fallen, on average, 1% per year for the past 10 years the HPV vaccine has been in use. In vaccinated women in this age group, this number should be reduced by at least 50% for an incidence of 0.7 per 100,000 women. This means that only 7 out of every 1,000,000 women who have been vaccinated against HPV will develop cervical cancer.
The HPV vaccine can help prevent cervical cancer while the introduction of HPV testing to Pap smears has enabled more women to receive treatment of pre-cancerous lesions. Co-testing has also enabled women to receive fewer unnecessary tests without increasing their risk. Cervical cancer is a preventable and treatable condition, and these measures will help decrease the number of women who develop cervical cancer.
Medical Reviewer: Michael Ferraro, MD, is an associate dean for TCMC’s South (Wilkes-Barre) Regional Campus and a practicing gynecologist.
Sources: Centers for Disease Control, Journal of Infectious Diseases, National Cancer Institute.
Read Dr. Mackarey’s Health & Exercise Forum – every Monday in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Dr. Daniel Shust
Guest Columnist: Dr. Daniel Shust, 2015 Doctor of Medicine Graduate from The Commonwealth Medical College (TCMC)
Daniel Shust, MD., is originally from Greenfield Township. He received his Bachelor of Science (BS) in Biopsychology from Penn State in 2005, a Master of Biomedical Sciences (MBS) from The Commonwealth Medical College (TCMC) in 2010 and a Doctor of Medicine (MD) from TCMC in 2015. Currently, Dr. Shust is a resident in The Wright Center’s Regional Family Medicine Residency Program, based in Wilkes Barre, PA.
One of the greatest frustrations in modern medicine occurs when a safe, tried and proven treatment exists to prevent deadly disease but it is not possible to administer it to the potentially vulnerable victims. Unnecessarily, overtime the disease spreads exponentially. Malaria in sub-Saharan Africa where one million die from the disease each year and tuberculosis in Haiti where the highest rates in the Western Hemisphere exists, are two examples. More recently, parents in California have made national news because they refused to vaccinate their children from measles. Since the measles vaccine was introduced in 1963, a 99 percent reduction has been attained. However, as of last month, 79 confirmed cases of measles in California due to parent refusal to vaccinate their children due to unsubstantiated fear of harm to their children.
The vast majority of parents belonging to the “anti-vaccine movement” justify their actions with completely unfounded and unsupported fears of autism and other illnesses from the vaccine. However, their decisions affect the health of not only their children, but others as well. The outbreak has quickly spread to Arizona, Utah, Washington, Colorado, Oregon, and Nebraska.
Another such disease that can be prevented with vaccination is the Human Papillomavirus, (HPV). Some strains of HPV lead the cancer. A 100% percent disease prevention rate is associated with those vaccinated before the age of first potential exposure.
According to Paul Offit, MD, professor of pediatrics, division of infectious diseases director of the Vaccine Education Center at the Children’s Hospital of Philadelphia (CHOP), every year in the United States, thousands of men and women die of cancers that can be prevented with a simple vaccine administered during adolescence to prevent HPV. He states, “It is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
The Centers for Disease Control (CDC) has listed the prevention of HPV as a one of its “Top 5 Health Initiatives.” The pressure will be on health care providers to take time educate and dispel myths in order for parents to make informed decisions for the health of their children. In fact, local pediatrician Anders Nelson, who spends significant time educating parents and children about the importance of vaccination, requires parents to sign a “Refused HPV Vaccine” form and boasts a 99% compliance rate.
2013 the CDC reported 13.9% of males and 37.6% of females’ ages 13-19 are completing vaccination for Human Papillomavirus (HPV). Despite such low vaccination rates, a 50% reduction in HPV among 14 -19 year old females is note. Moreover, studies demonstrate a 100% success rate to eradicate HPV in children vaccinated between the ages of 9 and 11 years old. With this in mind, health professionals ask a frustrating and burning question: “Why do parents hesitate to vaccinate their children from a potentially deadly virus when a safe and effective cure exists?”
Reasons cited by parents for not vaccinating are challenging to health providers. Some of the most common responses include misunderstanding of HPV and its impact, unfamiliarity with vaccine recommendations, distrust of vaccine safety, religious and moral issues with mode of disease transmission, and social pressures. It will be the purpose of this column to dispel myths and address these concerns among parents.
HPV is the most common sexually transmitted disease (STD) in the United States. It is estimated that nearly all sexually active Americans will at some point become infected with the virus. HPV is spread by direct skin to skin contact. Although the infection maybe asymptomatic, it is still possible to spread the virus. Condoms are not 100% effective to prevent HPV because infected skin may be present outside of the barrier.
Studies have demonstrated that at any given time, 52.8% of males will be infected. American females’ infection rates vary primarily with age. Although the prevalence of the disease among all females age 19-59 is 26.8%, females age 20-24 have a prevalence of 44.8%.
HPV is a family of viruses that primarily produce warts, but a limited number are responsible for cancers. There are a total 120 different subtypes of the virus capable of producing warts on skin or mucus membranes. Specific strains of the virus show preference for sites of infection, and different disease progressions. For example, most types are responsible for common warts on the hands and feet, however, there are strains with a preference for producing genital/anal disease. Moreover, the HPV causing the most of significant concern are those strains responsible for certain cancers. Some HPV strains will directly interrupt a cells repair cycle, resulting in vulnerability to be transformed into a cancerous cell. HPV types 16 and 18 are high risk for cancer and account for 70% of all 490,000 cases cervical cancer with 3,900 deaths. In addition, these two types cause penile, anal and head/neck cancers.
Prevention is paramount because once infected there is no treatment for HPV infections. Only the associated lesions, including genital warts, recurrent respiratory papillomatosis (RRP), pre-cancers, and cancers are treated. Treatment options professionals utilize are biopsy, cauterization, cryotherapy, and can be mildly to severely disfiguring. Biopsy results are used to determine the HPV strain and treatment. High risk subtypes lead to increased medical observation, and have the potential for more invasive treatments which can impair fertility and cause facial disfigurement.
The two vaccines available for use are Gardasil and Cervarix. Both vaccines protect against HPV 16 and 18, which account for 70% of all cervical cancers. Gardasil additionally protects against other high and low risk virus types.
The Gardasil vaccine was initially developed in the mid 1980’s at various institutions in the US and abroad. HPV proteins were added to a previous vaccine base that was proved safe and effective. After 20 years of testing and scrutiny by the FDA, Gardasil was deemed safe and released to the public in 2006.
Since distribution of the Gardasil vaccine, 67 million were administered with less than .037% adverse events. The reported vaccine reactions are injection site discomfort, dizziness, and fainting. Furthermore, research has concluded that there is no association with neurological conditions such as Guillain-Barre’ and Autism.
Gardasil and Cervarix are licensed for use for males and females ages 9 through 26 years. The vaccines are administered in a series of three on a 0, 2, and 6-month schedule. Studies have shown vaccination earlier in the recommended age spectrum has more advantageous results. For example, children administered the vaccine between the ages of 9-11 display 100% prevention of disease. Sexually activity is not a contraindication to receiving the vaccine, but the vaccine is not recommended to those currently pregnant.
Despite the safety and efficacy of the vaccines, one reason reported by parents for not vaccinating their children is the concern that vaccination will increase sexual activity in adolescents. Although disconcerting for parents, a study conducted two years before the introduction of Gardasil by the U.S. Department of Health and Human Services reported that the number of sexually active teens has increased to 30% in ages 15 to 17 and more than 63% in ages 18 to 19. Furthermore, these numbers continued to increase regardless of public programs in sexual education and abstinence.
Since released in 2006, Gardasil has made a direct impact on HPV prevalence in adolescents. Even with vaccination rates of 37.6%, HPV prevalence among adolescent females age 14-19 is 50% less than previously recorded. The decline in affected teens is predicted to lead to decreased future HPV related cancers. These vaccinations are safe, effective, powerful tools at our disposal to protect our children from the detrimental effects of a preventable disease. If you would like more information on Gardasil or Cervarix consult your local Family Physician, Pediatrician, or Obstetrician-gynecologists (OB/GYN).
Remember the advice of CHOP pediatrician, Dr. Paul Offit regarding the HPV vaccination for adolescents, “it is critical that doctors and parents keep in mind; the disease is NOT ABOUT SEX…IT IS ABOUT CANCER!”
Read Dr. Mackarey’s Health & Exercise Forum – every Monday in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Guest columnist: Sarah Singer, BFA, PTA
Spring has sprung and so too has Tour de Scranton, considered the “kick off” to biking season in NEPA. So, dust off your bikes and warm up for the event by riding the many beautiful and well-maintained trails are available at the Countryside Conservancy at Lackawanna State Park, other locations in the Abingtons or the Lackawanna Heritage Valley Authority.
Whether you take part in the Tour de Scranton or head out for a few easy miles later in the season, ensuring a proper bike fit should be on your checklist. Riding a bicycle that is properly fit to your style and body will not only help to prevent injury, but allow for a more comfortable riding experience. There are many things to take into consideration when checking your bike fit. First and foremost you must choose a bike that fits your style of riding.
For the sake of simplicity 3 basic styles of bikes include Road bikes, Hybrid bikes and Mountain bikes. Road bikes are designed for long distance riders, hybrid bicycles can be used for longer distance riders, but usually accommodates a recreational cyclist, and mountain bikes are designed for dirt or gravel and technical trails. The next component of ensuring a proper bike fit is making sure that you have a good foundation by choosing the right sized frame. To find the right sized frame you can use the following guidelines as a way to start or simply ask the local bike shop or bike fit consultant of your choice for help.
Road bikes: When straddling the bike you should have about 1” of clearance between your body and the top tube if the bike has a straight top tube (which runs parallel to the ground). When lifting the bike you should have 1” clearance between the tires and the ground. If the bike has a sloping top tube (semi-compact design) you should have a clearance of 2” or more.
Mountain bikes: When straddling the bike lift the bike off the ground and you should have a minimum of 2” clearance between the ground and the tires. With full suspension bikes you will want 1”-2” standover clearance because when you sit on the bike the frame will become lower from compressing the suspension. More aggressive riders will likely have 3”-5” of clearance.
Comfort bikes: Standing over a comfort bike to chose the right sized frame is not necessary. They are commonly designed with a steep sloping top tube and allow the rider to put feet firmly on the ground when the rider comes to a stop.
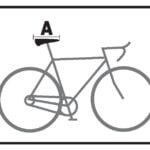
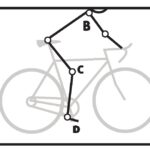
Now that you have right size for your bike you should adjust the components of the bike to allow for a more comfortable riding experience. Please use the diagram as a point of reference for the following tips. Also be sure to reexamine your bike fit after any bad falls. Keep in mind these measurements are meant to be used as a simple guideline and if you have any pre existing injuries or concerns please be sure to consult your local Physical Therapist or bike fit consultant.
Seat/Saddle
Your Seat or saddle should be level (See “A” on diagram). If it is tilted too far forward there will be too much weight on hands, arms and lower back. If it is too far backward, there may be strain on LB and may lead to saddle related pain.
Your knee should be measured at the most extended position to adjust saddle height. (see “Knee to Pedal”)
The saddle should be a comfortable distance from handlebars. If it is too close it will place too much weight on your mid-back and arms. If it is too far it will put extra strain on your low back and neck. Also make sure seat is the proper width to ensure a more comfortable ride.
Handlebars (HB)
Your handlebar placement will affect your hands, shoulder, neck and back. The higher the handlebars are the more weight is placed on the saddle. Taller riders should have lower handlebars in relation to height of saddle
For road cyclists there should be a 90° angle between your arm (near the shoulder) and your trunk with a slight bend at your elbows of about 15° (See “B” on diagram).
Your trunk angle should be 25-35° if you are a road bike cyclist and 35-90° comfort/recreation cyclist
Knee to Pedal
The knee to pedal measurement should be taken with the knee in the most extended position. There should be about a 25-35° angle at the knee (See “C” on diagram)
Foot to Pedal
The ball of your foot should be over the pedal spindle (See “D” on diagram). This will allow for the best leverage, comfort and efficiency. Using a stiff soled shoe is recommended.
Even if you are a recreational cyclist it’s a good idea to take all the proper steps in preventing injury. This article can be used as a reference point to help to prevent common cycling injuries, enhance your comfort and improve your riding efficiency. If you have any further questions about enhancing your bike fit please contact your local physical therapist or bike fit consultant.


Sources: REI.com, APTA.org
Illustrations: Sarah Singer; Model: Brittany Ostrowski
Guest Columnist: Sarah Singer, BFA, PTA is a physical therapist assistant at Mackarey Physical Therapy, specializing in orthopedic and sports rehab.
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, and exercise regularly
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice in downtown Scranton and is an associate professor of clinical medicine at The Commonwealth Medical College.
HIP FRACTURE PREVENTION – PART 2 of 2
Injuries due to falling are a very common problem in the elderly. Hip fractures are the most common injury due to falling in the seniors. According to the American Academy of Orthopaedic Surgeons, each year more than 300,000 people are hospitalized for hip fractures in the United States. These fractures represent 72% of all fracture costs, totaling more than 12 billion dollars in 2005 and, not surprisingly, 90% occurred in those 65 and older. Most hip fracture patients who previously lived independently will require family assistance, home or long term care and 50% will require a cane or walker.
A recent study by the American Physical Therapy Association found that patients benefited from a physical therapy evaluation to determine their risk level for falling. If a high-risk level is found on a falls assessment, physical therapy interventions can be successfully employed to improve strength, balance, and coordination and falls prevention. Also, a well-balanced diet, exercise, Calcium with vitamin D supplements and medications can help prevent or retard osteoporosis and prevent hip fractures.
EXERCISES TO PREVENT HIP FRACTURES:
***Always perform slowly, alternate right and left sides, limit other distractions and concentrate on the exercise to retrain the brain, 10-20 times each 2-3 times per day.
***Caution: Do not do standing exercises without assistance or supervision if needed
Standing Hip Hikes (photo 1)
Face a countertop and hold onto it with both hands. Hike your hip and knee up to 90 degrees as if you are marching. Hold the position for 3-5 seconds on one leg and lower slowly. Repeat this on the other leg and alternate 10 times.
Standing Hip Scissor Kicks (photo 2)
Face a countertop and hold onto it with both hands. Lift your leg up 30 degrees as if you are spreading your legs apart. Hold the position for 3-5 seconds on one leg and lower slowly to cross over the middle. Repeat this on the other leg and alternate 10 times.
Standing Squats (photo 3)
Face a countertop and hold onto it with both hands. Bend your hip and knee down to 45 degrees to a squatting position. Hold the position for 3-5 seconds on both legs and return to standing slowly. Repeat this 10 times. Once strong enough try on one leg at a time and alternate.
Chair Squats (photo 4)
Sit in a chair with arm rests. Get out of chair only using your legs. Hold the position for 3-5 seconds and return to sitting. If necessary, use 1 or 2 arms to assist. Repeat this 10 times. Focus on trunk core stabilization and leg strength. Use more leg muscles and less arm muscles as strength improves.
Line Walk (photo 5)
Place a straight line on the floor and practice “walking the line” with the right then left foot on the line.
Single Leg Stance (photo 6)
Hold onto a chair while bending one knee and shifting your weight to the other leg. Hold for 3-5 seconds and repeat with the other leg. Increase time 10 -15 -20 seconds as tolerated.






If you feel you or a loved one may be at risk for falling or a hip fracture, ask your family physician if a physical therapy consultation for a falls prevention program to prevent hip fractures may benefit you.
Model: Sarah Singer, PTA
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 1 of 2
My father celebrated his 91st birthday this January in a hospital bed due to a recent fall. While, it didn’t stop us from enjoying cake and ice cream, it did limit his mobility. He enjoyed 90 wonderfully active years; however, his independence was lost the same way more than one-third of a million people lose their independence each year… hip fractures! As a doctor of orthopedic physical therapy, I feel remise that I could not prevent this from happening to my father. What most of us fail to realize is that his fracture, like many, was more than just an orthopedic problem …it involves age, gender, diet, exercise, vision, leg strength, medications, environmental risks, and vestibular problems (inner ear problems effecting balance).
Injuries due to falling are a very common problem in the elderly. Hip fractures are the most common injury due to falling in the seniors. According to the American Academy of Orthopaedic Surgeons, each year more than 300,000 people are hospitalized for hip fractures in the United States. These fractures represent 72% of all fracture costs, totaling more than 12 billion dollars in 2005 and, not surprisingly, 90% occurred in those 65 and older. Most hip fracture patients who previously lived independently will require family assistance, home or long term care and 50% will require a cane or walker.
Several risk factors for hip fractures have been identified. While some factors are somewhat controllable and may improve bone quality, (diet, exercise, smoking, alcohol) others are not.
Hip Fracture Risk Factors:
Preventing a fall can not only save your independence but also your life! Preventing injuries from falls reduces the need for nursing home placement.
Tips to Prevent Falls/Fractures:
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune: Hip Fractures - Part 2 of 2
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Christopher A. Peters, M.D.
MARCH IS COLON CANCER AWARENESS MONTH!
TCMC “Wisdom of Well-being”
Guest Author: Christopher A. Peters, M.D, NROC/TCMC/NRCI
Dr. Christopher Peters is a partner of Radiation Medicine Associates of Scranton (RAMAS) and serves as medical director of Northeast Radiation Oncology Centers (NROC). He is the director of clinical research at NROC, and serves as the Principal Investigator for NROC's full member status in the Radiation Therapy Oncology Group (RTOG). In 2012, Dr. Peters joined the board of directors of the Northeast Regional Cancer Institute (NRCI). He is an Associate Professor of Medicine at The Commonwealth Medical College (TCMC) and Director of the fourth-year TCMC elective in radiation oncology.
In 2000, President Bill Clinton dedicated March as National Colorectal Cancer Awareness Month. The purpose of this designation is to increase public awareness of the facts about colon cancer – a cancer that is preventable, treatable and has a high survival rate. Regular screening tests, expert medical care and a healthy lifestyle, which includes a proper diet and exercise, are essential for prevention. Several studies have demonstrated that exercise can also help prevent colon cancer.
The American Cancer Society estimates that approximately 136,830 people were diagnosed with colorectal cancer in 2014. Of these, 50,310 men and women will succumb to the disease. It is the second-leading cause of U.S. cancer deaths for both men and women combined. The good news is incidence and mortality rates are dropping both nationally as well as in northeast Pennsylvania. The bad news is northeast Pennsylvania still has increased incidence and mortality rates when compared to the national average.
Studies show that prevention of this disease is multifaceted and includes: engaging in daily exercise, eating a low-fat diet with little red meat, avoiding smoking, drinking in moderation and having regular colonoscopy screenings.
Early detection is the key to survival. Death from colorectal cancer can be eliminated if caught at the earliest signs of disease. Colorectal cancer progresses very slowly, usually over years. It often begins as non-cancerous polyps in the lining of the colon. In some cases, these polyps can grow and become cancerous, often without any symptoms. Some symptoms that may develop are: blood in stool, changes in bowel movement, feeling bloated, unexplained weight loss, feeling tired easily, abdominal pain or cramps, and vomiting. Contact your physician if you have any of these symptoms.
The risk of colon cancer increases with age, as 90 percent of those diagnosed are older than age 50. A family history of colon cancer increases risk. Also, those with benign polyps, inflammatory bowel disease, ulcerative colitis or Crohn’s disease are at greater risk and should be screened more frequently.
Prevention of Colon Cancer:
How Exercise Prevents Colon Cancer:
The intestine works like a sewage plant, recycling the food and liquid needed by your body. However, it also stores waste prior to disposal. The longer the wastes remain idle in your colon or rectum, the more time toxins have to be absorbed from you waste into the surrounding tissues. One method in which exercise may help prevent colon cancer is to get your body moving, including your intestines. Exercise stimulates muscular contraction called peristalsis to promote movement of waste through your colon.
Exercise to prevent colon cancer does not have to be extreme. A simple increase in daily activity for 15 minutes, two times per day or 30 minutes, once per day is adequate to improve the movement of waste through your colon. This can be simply accomplished by walking, swimming, biking or playing golf, tennis or basketball. For those interested in a more traditional exercise regimen, perform aerobic exercise for 30-45 minutes four to five days per week, with additional sports and activities for the remainder of the time. For those in poor physical condition, begin slowly. Start walking for five to 10 minutes, two to three times per day. Then, add one to two minutes each week until you attain a 30-45 minute goal.
Source: American Cancer Society/Northeast Regional Cancer Institute, and CA Cancer J Clin.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
New Research
It is a well established fact in the medical literature that the benefits of regular exercise and physical activity are numerous, from reducing blood pressure to lowering the risk of falls. (SEE "LIST A" BELOW) However, a study recently published in the Journal of Physiology reports that aerobic exercise may improve brain health and be more effective than other types of exercise in stimulating new brain tissue.
The relationship between exercise and neurogenesis, the formation of new brain cells in the adult brain, has been studied for many years. Previous studies have reported an association between exercise and increased brain size and density when compared to those who are more sedentary. However, until recently, it has been unclear exactly which form of exercise is most effective in the formation of new brain cells in the adult brain. Recent animal studies compared the effects of three popular forms of exercise on the brain; aerobic exercise, high-intensity interval training, and resistance weight training.
Subjects were divided into one of four groups; sedentary (control group), aerobic exercise, (moderate intensity distance running), high-intensity interval training (strenuous running for 3 minutes followed by 2 minutes slow jog with repetitions for 15 minutes), and traditional resistance weight training for seven weeks. Brain tissue was examined microscopically before and after the seven weeks. Results showed that the levels of new neurons in the brain were significantly greater in the aerobic exercise group (sustained distance running) when compared to all other groups; sedentary, interval and weight training. While the interval high-intensity training group had slightly higher levels of new neurons than the sedentary group, it was significantly less than the aerobic group. The weight training group, while stronger, did not produce new neurons in the brain.
What is Aerobic Exercise?
In this study, aerobic exercise was in the form of distance running. However, in a broader sense, aerobic exercise is any type of sustained exercise that strengthens the heart and lungs to improve the body’s use of oxygen. This may include running/jogging, brisk walking, cycling, swimming, rowing, and the use of a treadmill, elliptical, stepper or similar device, at light to moderate intensity which requires the use of oxygen to adequately meet the oxygen demands of the body for an extended period of time. The generally accepted time and frequency is at least 30 minute sessions performed three or more times per week.
Summary
Researchers conclude that, while further research is required, the application for humans may prove extremely valuable. However, at this point; it is not clear why the aerobic group significantly produced new neurons when compared to the others. The moderate but prolonged demand for oxygen to the brain is thought to be linked. They caution exercise enthusiasts not to take the results out of context. It is recommended that people engage in comprehensive exercise programs which incorporate all aspects of health and wellness. (SEE " LIST B" BELOW)
A comprehensive exercise program includes:
SOURCES: Journal of Physiology Feb 2016; wikipedia.org
LIST A: Some of the more important benefits of exercise are:
LIST B: Some simple suggestions for beginning an exercise program are:
Visit your doctor regularly and listen to your body. Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Steven Scheinman, M.D.
MARCH IS NATIONAL KIDNEY MONTH!
Guest Author: Steven J. Scheinman, M.D., President and Dean of The Commonwealth Medical College
Your heart counts on normal levels of potassium to maintain normal rhythm. Your muscles produce chemical waste as they work. Sodium influences blood pressure. Excretion of water and salts needs to match intake. Scores of delicately balanced, intricately interconnected chemical exchanges power a single healthy body. At the center of this exquisite dance, regulating chemical levels and removing the waste, are your kidneys.
March is National Kidney Month and a good time to recognize how important kidneys are to our health and how costly and debilitating it is when they fail. According to the United States Renal Data System, in 2013 Medicare spent $28.6 billion on hemodialysis, the last resort of patients with renal disease. While the monetary cost is enormous, kidney disease also takes a heavy toll on quality of life. There have been wonderful advances in both dialysis and the kidney transplantation, but both still carry an onerous burden. Dietary and, sometimes, travel restrictions accompany dialysis. Post-transplant patients face a lifetime of meticulous adherence to medication regimens that include multiple, often expensive, drugs.
As is the case with many diseases, prevention of kidney disease is far preferable to treatment. To preserve kidney health, it’s important first to recognize the causes of kidney disease. Long-time use of certain drugs, including NSAIDs like ibuprofen, can cause kidney failure. So can many autoimmune disorders. There are genetic causes, such as polycystic kidney disease. Certain cancers are also implicated. However, diabetes is by far the No. 1 cause of kidney failure. Hypertension itself is another major cause. Further, hypertension will accelerate the progression of renal disease no matter the cause. Everyone should take their blood pressure very seriously, and particularly if you have signs of kidney problems.
At its advanced stage, signs and symptoms of kidney disease include puffiness around the eyes, swelling of the ankles and blood in the urine. Weakness and fatigue are also common because kidney disease causes anemia. Healthy kidneys produce a hormone called EPO, which stimulates the bone marrow to make oxygen-carrying red blood cells. When the kidneys are diseased or damaged, EPO levels drop and anemia results. Dry and itchy skin, and muscle cramping, may arise from electrolyte imbalances caused by poorly functioning kidneys The National Kidney Foundation (NKF) advises patients to look for foamy urine. This foam, NKF says, “may look like the foam you see when scrambling eggs, as the common protein found in urine, albumin, is the same protein that is found in eggs.”
These signs and symptoms sound dramatic, but most do not occur early on, and kidney disease too often goes undetected until its late stages. That’s unfortunate because once the kidney damage has progressed it is too often irreversible. There are simple tests to check kidney health that should be part of every adult’s routine health maintenance.
The purpose of blood and urine tests isn’t to alarm but to arm. Information is a powerful weapon deployed in in the service of prevention. Everyone should strive to maintain a healthy weight and get adequate amounts of exercise, but this advice is particularly important if you have early warning signs of an unhealthy blood pressure or diabetes. The good news is that mild cases of diabetes and high blood pressure respond well to lifestyle changes. If you have high blood pressure or diabetes, it’s vital to follow your doctor’s advice and take medicines as prescribed. Know your numbers, take care of yourself, comply with medical advice and keep your kidneys working properly.
Guest Author: Dr. Scheinman is a nephrologist and president and dean of The Commonwealth Medical College, with campuses in Sayre, Scranton, Williamsport and Wilkes-Barre.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
