
Dr. Peter Cognetti
Guest Author: Peter Cognetti, MD, practices family medicine in Scranton and is regional education coordinator, family medicine for The Commonwealth Medical College’s North Campus in Scranton.
This column is a special feature the third Monday of every month of Health & Exercise Forum in cooperation with The Commonwealth Medical College.
DEHYDRATION: SPECIAL CONSIDERATIONS FOR THE ELDERLY
Summer heat is here and the risk of dehydration continues for one specific group, the elderly. Age, diet, illness and medications are some of the many reasons why elders suffer from dehydration not only in the summer heat, but year round.
Next to oxygen, water is the nutrient most needed for life. A person can live without food for a month, but most can survive only three to four days without water. Even though proper hydration is essential for health, water gets overlooked as one of the six basic nutrients. Dehydration occurs when the amount of water taken into the body is less than the amount that is being lost. Dehydration can happen very rapidly (i.e. in less than eight hours); the consequences can be life threatening and the symptoms can be alarmingly swift.
In the body, water is needed to regulate body temperature, carry nutrients, remove toxins and waste materials, and provide the medium in which all cellular chemical reactions take place. Fluid balance is vital for body functions. A significant decrease in the total amount of body fluids leads to dehydration. Fluids can be lost through the urine, skin, or lungs. Along with fluids, essential electrolytes, such as sodium and potassium, are also perilously depleted in a dehydrated individual.
Dehydration is the most common fluid and electrolyte disorder of frail elders, both in long term care facilities and in the community! Elders aged 85 to 99 years are six times more likely to be hospitalized for dehydration than those aged 65 to 69 years. More than 18% of those hospitalized for dehydration will die within 30 days, and associated mortality increases with age. Men appear to dehydrate more often than women and dehydration is often masked by other conditions.
Elderly individuals are at heightened risk for dehydration for several reasons. Compared to younger individuals, their regulatory system (i.e. kidneys and hormones) does not work as well and their bodies have lower water contents. The elderly often have a depressed thirst drive due to a decrease in a particular hormone. They do not feel thirsty when they are dehydrated. This is especially true in hot, humid weather, when they have a fever, are taking medications, or have vomiting or diarrhea. They have decreased taste, smell, and appetite which contribute to the muted perception of thirst. Because of dementia, depression, visual deficits, or motor impairments, elderly persons may have difficulty getting fluids for themselves. Many elderly individuals limit their fluid intake in the belief that they will prevent incontinence and decrease the number of trips to the bathroom. The medications that they are taking (e.g. diuretics, laxatives, hypnotics) contribute to dehydration.
Elders may suffer headaches, fainting, disorientation, nausea, a seizure, a stroke, or a heart attack as a result of dehydration. The minimum daily requirement to avoid dehydration is between 1,500 (6.34 cups) and 2,000 ml of fluid intake per day. Six to eight good-sized glasses of water a day should provide this amount. Better hydration improves well-being and medications work more effectively when an individual is properly hydrated.
Those who care for the elderly whether at home or in a health care facility need to be alert to the following symptoms:
Plain old tap water is a good way to replenish fluid loss. Some energy drinks not only have excess and unneeded calories but also contain sugar that slows down the rate at which water can be absorbed form the stomach. Consuming alcoholic and caffeinated beverages actually has an opposite, diuretic effect!
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
 It is the time of year when many runners will ramp up their training for the Steamtown Marathon to be held in October. As you increase your mileage in preparation for the marathon you probably have noticed some difficulty walking down the steps for your morning coffee the next morning. The stiffness in your joints, coupled with severe muscle soreness, makes you walk like an arthritic octogenarian. In spite of stiff hip, knee and ankle joints you should feel good about your accomplishment. I am sure that your well-meaning wife, parents, friends, and coworkers, (especially those who don’t like to run) are telling you how foolish you are to run 26.2 miles. They will say that you are ruining your knees and it is time to grow up. Many will say that you will regret this someday when you can’t even walk without pain.
It is the time of year when many runners will ramp up their training for the Steamtown Marathon to be held in October. As you increase your mileage in preparation for the marathon you probably have noticed some difficulty walking down the steps for your morning coffee the next morning. The stiffness in your joints, coupled with severe muscle soreness, makes you walk like an arthritic octogenarian. In spite of stiff hip, knee and ankle joints you should feel good about your accomplishment. I am sure that your well-meaning wife, parents, friends, and coworkers, (especially those who don’t like to run) are telling you how foolish you are to run 26.2 miles. They will say that you are ruining your knees and it is time to grow up. Many will say that you will regret this someday when you can’t even walk without pain.
Up until recently, your well-intended family and friends had reason to be concerned. Many previous studies indirectly supported their point of view. A British study found that almost 50% of former elite soccer players had crippling, bone-on-bone knee arthritis by middle-age. Similar findings were reported for elite weight lifters and retired NFL football players. However, the good news for runners is that they may be different. The lean, light-weight runner, who trots like a deer, light on his feet, in perfect alignment, and with good form, may not be doing so much damage to his knee joints after all.
Therefore, I hope to add to some level of comfort as you prepare for a 26.2 mile journey by sharing wonderful news based on recent research about runners and knee arthritis. You may not have done as much damage to your joints as previously theorized. Last year an article in Skeletal Radiology received significant attention for disproving “current wisdom” about running and knee arthritis. Researchers from Austria used MRI imaging to examine the knees of participants before the 1997 Vienna Marathon. Ten years later, runners received an MRI before the 2007 race. Scans of those participating in both races were compared for changes. The results were very surprising. No major changes regarding new internal damage to the knee joints of the runners in both marathons were discovered.
A 2008 Stanford University study supported the findings in the Austrian study. In 1984, Stanford researchers followed runners who began running in their 50’s and 60’s and continued to run for 20 years and compared them to the same age group of non runners. While 7% of the runners began the study with creaking and crackling associated with mild arthritis under the knee caps, none of the non runners had such findings. However, 20 years later, only 20% of the runners had advanced arthritic changes compared with 32% of the control group. Furthermore, only 2% of the runners had knee arthritis requiring surgery when compared to 10% for the control group.
Therefore, current wisdom suggests that running may not cause advanced and progressive knee arthritis. Moreover, running may actually offer protection by grooving the surfaces through motion and creating demands on the cartilage in the joint to rebuild, repair and protect. Keep in mind that the joint requires optimum conditions to benefit from the stresses associated with running. Some suggestions purported are:
Top Ten Suggestions for Running with Healthy Joints
Remember, not every workout has to be pounding and demanding
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
“The woods are lovely, dark, and deep,
But I have promises to keep,
And miles to go before I sleep,
And miles to go before I sleep.” Robert Frost
The purpose of this column is to present an alternative to traditional running that will allow training on more interesting and less stressful surfaces such as those used when hiking, mountain biking and horse riding trails in the beautiful woods of Northeast Pennsylvania.
Summer is in full gear as many of us seek to find new and exciting outdoor activities. While I am not pounding the pavement like I used to, I often reflect on my favorite running moments. One hot fourth of July, I was at a family picnic at Lackawanna State Park and decided to go for a run. As I set out on State Road 348, the sun was beating down on me. I happened to see a sign that read, “Orchard Trail, Bull Hill Trail, Tree Line Trail.” I thought it might be a good idea to find some shade and decided to run on this path normally used for hiking, mountain biking and horseback riding. It turned out to be a great decision. While I was forced to run 25% slower due to the uneven terrain, I was able to practice “light running” techniques by running with short strides on the balls of my feet. I felt much more refreshed as I avoided the direct sunlight under the cover of the trees. Furthermore, I enjoyed the up close view of nature as I ran by cool streams and wet mossy rocks. I saw beautiful flowers, rhododendron, and mountain laurel. I observed deer, chipmunks and birds. In my quest to avoid the hot sun, I discovered the beautiful underworld of “trail running” – a growing trend in today’s running community. If you, like me, have been running for many years, trail running can help you rediscover why you love to run. It is beautiful, peaceful, natural and unique. It is fun to get in touch with your inner child as you run in the woods and get muddy. Trail running is not only a good form of cross-training it also makes running fun!
The trail running community purports that trail running is popular because it satisfies a primal need for man to move through nature, derived from hunter/gatherer days. Others who promote trail running feel the popularity is due to the many advantages it offers. One, trail running prevents impact injuries due to soft surfaces. Two, the training style of running with shorter strides on the ball of the foot, lessens impact. Three, this type of running will develop stronger ankles and trunk core muscles while improving balance, coordination and proprioception from running on uneven surfaces. Lastly, the ability to release copious amounts of endorphins while breathing fresh air instead of roadside fumes is invaluable.
Clothing - Trail running clothes can be the same as those worn for road running except be sure you don’t mind if they get dirty and a little torn or snagged.
Shoes – While you can begin trail running in the same shoes you road run in, you will find that a different pair is necessary due to excess dirt and water. Also, if you decide to get into trail running, it is worth purchasing trail shoes which are stronger, more water proof and offer better traction.
Water – a hand held water bottle or a water bottle belt is essential. The belt offers little pouches for money, keys, ID, and power bars for longer runs.
Insect Repellent - a must
Headlamp – necessary for evening runs because it gets very dark in the woods. Also, it gets dark earlier in the woods than on the roads and you need to see the terrain clearly.
Change of Clothes – it is a good idea to have a first-aid kit, towel and change of clothes in your car to change into before you drive home.
Find a Trail – Start by asking around. Hikers, mountain bikers, and horseback riders are a good start. The American Trail Running Association has a website with a free directory of trails in the United States. PA State Parks such as Lackawanna State Park in Dalton, offer many options (www.visitPAparks.com). Learn the difference between “non technical trails” which are wider with a paved, dirt or gravel base and much easier than “technical trails” which are narrow, rocky, hilly and challenging.
Run Slowly – To be safe, run 25% slower when running a trail in the woods. Use a short stride and land on the ball of your foot. Forget about the pace, feel the dirt under your feet, work on balance and stability. It is a different type of running.
Walk – Don’t hesitate to walk when necessary, especially up rocky and slippery hills.
Keep Your Eye on the Trail – Pay careful attention to the terrain by looking 5 to 10 feet ahead.
Anticipate Slippery Rocks and Stumps - Pick your feet up higher and bend your hips and knees more when necessary to avoid tripping over a log. Walk over obstacles if necessary.
Keep a Distance – Don’t crowd the trail. You may have to share it with other runners, bikers and hikers. Pass with care.
Be Safe/Be Prepared– Remember the first-aid kit, cell phone, extra clothes and food in the car and make sure someone knows where you plan to run. Run with a friend.
Sources: American Trail Running Association, Trailspace.comVisit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum" in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of medicine at The Commonwealth Medical College.
According to the Centers of Disease Control (CDC), Hypertension (HTN), also known as high blood pressure (HBP), affects one in three adults (67 million people) in the USA. Unfortunately, only one-half of those with high blood pressure control the problem and, as a result, are at great risk for heart disease and stroke. Emergency rooms in the United States have experienced a 25% increase in emergency room visits for HBP between 2006 and 2011.
Blood pressure numbers represent the force against the walls of your arteries. Normal blood pressure (BP) is defined as a systolic pressure (the top number) of 120 mm Hg and a diastolic pressure (the bottom number) of 80 mm Hg (120/80). The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure has classified blood pressure as follows:
Medical Conditions or Medications Contributing to HBP*
Almost everyone has had their blood pressure checked with a standard or automatic blood pressure cuff. Sometimes, when a problem is detected, a home blood pressure unit is recommended to track BP throughout the day.
For most people with HBP, there are no obvious symptoms. HBP is usually detected at a health fair or a routine visit with a physician. However, over time, HBP can cause problems with the heart and kidneys. Sometimes, a more serious condition can develop from very high blood pressure called malignant hypertension. Symptoms include; severe headache, nausea and vomiting, confusion, vision changes and nosebleeds. Notify your physician immediately if you develop these symptoms.
According to a recent long-term study, both men and women without a history of coronary artery disease or high blood pressure suffered from both diseases when they did not manage stress well. Those who allowed stress to upset them, (short fused and easily frustrated) had significant increases in cholesterol and blood pressure when compared with those who were more even-tempered and easygoing under stress.
Exercise combats HBP and maintains a healthy body weight. The key to success when it comes to improving your life with exercise is to develop a regular, consistent program. A good program must include aerobic exercise (walking, jogging, biking) for 30 minutes (or 15 minutes twice a day) 4-5 days per week and mild/moderated weight training 2- 3 times per week.
A low salt, low fat diet which includes: fish, fiber, grains, fruits and vegetables is essential. Moreover, take care to avoid the “Seven Deadly Sins for High Blood Pressure” (Zee News):
In conclusion, while HBP is a potentially serious medical condition, for most it is a controllable and preventable problem. Lifestyle changes such as diet, exercise and stress reduction have been found to be most effective.
SOURCES: Centers For Disease Control (CDC); American Heart Association (AHA), University of Pittsburgh Medical Center (UPMC), National Institutes of Health (NIH), Medline Plus, Zee News
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Allergy Season is in Full Bloom!
Guest Author: Joel Laury, MD, is a assistant professor of medicine at The Commonwealth Medical College.
Dr. Laury is board certified in allergy and immunology. He graduated from the Albert Einstein College of Medicine, in New York City and did his internship and residency in internal medicine at the Bronx Municipal Hospital Center. He completed his fellowship in allergy, asthma and immunology at the Albert Einstein College of Medicine and is in private practice in Scranton.

Joel Laury, M.D.
This column is a special feature the third Monday of every month of Health & Exercise Forum in cooperation with The Commonwealth Medical College.
Allergic Rhinitis
An allergy is the body’s immune system overreacting to something that is not harmful. People can be allergic to medicines, foods, pollens, animals, molds, latex rubber, and many other things. Allergic rhinitis, sometimes called hay fever or rose fever, happens when people have allergies in her nose. They may sneeze, get a stuffy nose, runny nose, itchy nose, and feel like to have a cold that does not get better.
Often, people with allergic rhinitis have itchy, watery eyes, known as allergic conjunctivitis, or may develop asthma. Some people may get rashes, such as hives (urticaria) or eczema (atopic dermatitis). More than 50 million Americans have allergic rhinitis, and over 17 million adult, and 7 million children, have asthma. (1) All allergic diseases, including food allergies, have been increasing rapidly over the past century.
It sometimes can be hard to tell whether someone is suffering from allergic rhinitis, a cold, a sinus infection, or other causes of nasal misery. Some people feel worse near perfumes, cleaning fluids, would smoke or cigarette smoke. Generally, a cold should go away in about a week.
There are 3 main parts to treating allergies. The first step is to be tested, so that people can avoid what they are allergic to. This is called environmental control, and there are no side effects to this.
The next step involves taking medicines. Many good allergy medicines are now over the counter, and might work as well as prescription drugs. Of course, these only work while you are taking them, and some may have side effects, such as drowsiness, or nose bleeds.
If people are still suffering, then allergy shots may be prescribed. These are more for long term relief, and are continued for months or years. After stopping, many people may do well for many years afterwards! Sometimes a reaction may happen after a shot - such as itching, redness, hives, or difficulty breathing. Recently, the FDA has approved some allergens for sublingual (under the tongue) immunotherapy. So far, only ragweed and grass pollens are FDA approved. These might be somewhat safer than shots, but also may be somewhat less effective. They have been used in Europe for years, but only were approved in the US last year.
TIPS FOR ATHLETES AND OUTDOOR ENTHUSIASTS WITH ALLERGIES:
Warm-up/Cool Down
Whether you have allergic respiratory problems from rhinitis or asthma, you many benefit from conditioning your airways with a 10 to 15 minute warm-up before and cool-down after the activity. This may serve to gradually prepare your lungs for an increased demand.
Hydrate
In addition to preventing dehydration on hot and humid days, constant hydration is very important for the athlete with allergies to prevent dry airways in athletes.
Guidelines for Athletes with Allergies from the National Athletic Trainers Association:
Educate Staff
Know the signs and symptoms of asthma (coughing, wheezing, tightness in chest, shortness of breath).
Plan for the Problem
Some schools have a file on each student athlete with a allergic or asthmatic problem which requires medication. The file includes information such as medical doctor release and instruction, emergency contacts and medications. Students must have their medications on hand before they can enter the field. The National Athletic Trainers Association recommends using a peak flow meter to monitor at risk players and can determine when a player can return to the field.
Practice in Climate Control
If possible, find an alternate practice facility with climate control for athletes at risk. Plan practices for these athletes when the pollen count is low. Check the newspaper or internet for pollen counts in your area. Training by the water, (ocean) where there is a breeze and less pollen is helpful.
Shower and change clothing immediately after being outdoors
Modify Workout: during a flare up, do less aerobic exercise to limit stress on respiratory system. Try strength training indoors instead.
Modify Environment: when pollen count is high, keep windows shut at home and in your car….use air-conditioning.
Keep pets out of your bedroom…especially when sleeping
Dry clothing in dryer…do not hang on clothesline outdoors
Source: http://acaai.org/news/facts-statistics/allergies; National Athletic Trainers Association
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Like many of you, I have always enjoyed the outdoors...walking, running, biking, hiking etc. However, recently, I have been more concerned about my safety, (getting older and more cautious) when doing these activities on the side of the road. Over the years, I have encountered several close calls while walking, running or biking on the road, especially while running into traffic and drivers quickly pull out to go right on red. Add to that, current drivers are being distracted by electronic devices.
Almost 15 percent of all motor vehicle injuries to people happened to those not in cars but while walking, running or biking on the side of the road. In fact, runners and walkers incurred over 70,000 injuries and 4,000 fatalities from accidents from motor vehicles according to the Centers for Disease Control (CDC). These statistics continue to increase as the number of distractions to drivers increases (phone calls, texts, etc). Consequently, walkers, runners and cyclists must be more aware than ever to prevent injury or death from motor vehicles.
Five high risk factors for walkers, runners and cyclists:
“Runner’s World” offers the following recommendations:
Notify Someone: Be sure to communicate...leave a note at home about where you plan to go and how long you plan to be out. In an emergency you can be located.
Protection: If your route is in a high crime area, avoid dawn and dusk, carry self-defense spray, exercise with a partner, leave jewelry at home and vary your route and routine.
Identification: Carry proper ID, a cell phone and emergency contacts.
Be alert: Don’t assume a driver sees you. Instead, assume that the driver can’t see you.
Bike path etiquette: Walkers and runners should stay on the right side of the path and pass on the left. Be courteous when walking with a partner to leave the left lane of the path open for runners and bikers. Cyclists should use the left lane to pass and alert walkers and runners when passing.
Face traffic: Except for cyclists, walking and running “into” oncoming traffic is best. It’s easier to see, and react to, oncoming cars. And cars will see you more clearly too.
Share the road: If traffic gets heavy, or the road narrows, be prepared to move onto the sidewalk or shoulder of the road. When walking or running into traffic, stay as far left as possible. When biking, favor the far right side of the road.
Be Visible: Wear high-visibility, brightly colored clothing. When out at dawn or sunset, reflective materials are a must. A lightweight reflective vest is a great option. Use a headlamp or handheld light so you can see where you're going, and drivers can see you. The light should be a bright LED or blinking red as drivers see blinking red as a hazard.
Use your ears to be safe: Avoid using iPods or wearing headphones—you need to be able to hear approaching vehicles. If you do use headphones, do so with the volume low with just one earbud in.
Caution on the hills or curves: When they crest hills, drivers' vision can suddenly be impaired by factors like sun glare or backdrops.
Beware of high-risk areas: Be extra cautious in areas like entrances to parking lots, bars, and restaurants where there may be heavy traffic.
Watch for early birds and night owls: At odd hours be extra careful. Early in the morning and very late at night, people may be overtired and not as attentive.
Be Courteous: At a stop sign or light, wait for the driver to wave you through—then acknowledge with your own polite wave. That acknowledgement will make the driver feel more inclined to do it again for the next walker or runner. Use hand signals (as you would on a bicycle) to show which way you plan to turn.
CYCLISTS :
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Source: http://www.runnersworld.com
This Summer Make Your Pool a Health Spa! Have Fun and Get in Shape!
Enjoy the recent Memorial Day Weekend heat wave by getting in the pool! Each summer in Northeastern Pennsylvania people open their pools for fun in the sun. However, this summer I urge you to look at your pleasure puddle in different light…a health spa! It may very well be the exercise of choice for many people. Many have discovered the benefits of moving their limbs in the warm water of a home pool following knee or shoulder surgery. Also, long distance runners who often look for cross training methods without joint compression and arthritis sufferers who are often limited in exercise choices by joint pain from compressive forces when bearing weight, can enjoy the buoyancy effects of water. These are good examples of the benefits or water exercise…aerobic and resistive exercise without joint compression.
Most doctors recommend some form of exercise with arthritis. Pain and fatigue are the most limiting factors for the person with arthritis. Pool exercise may be the answer. With proper technique, adequate rest periods, appropriate resistance and repetitions, water exercise can be very effective.
The following are some of the benefits of water exercise:
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
PART 2 of 2: SAVE YOUR JOINTS! Exercises You Should Avoid if You’re Over 50!
Why Change is Necessary with Age
For many years, I have repeatedly preached about the value of engaging in an active lifestyle throughout life. It is especially important to be active as one gets older in order to maintain mobility and independence. However, many take this advice to an extreme and refuse to accept the inevitable changes that occur in the body with age. They run, jump, lift and throw like a teenager and often fail to modify their activity or exercise regimen appropriately for their age. Consequently, they suffer from multiple injuries, including muscle tears, tendonitis, bursitis, impingement and advanced osteoarthritis. Keep in mind, everyone ages differently. One person at 60 years of age may be the equivalent of another at 50. However, change with age is inevitable, so be kind to your body…it’s the only one you have! It is always prudent to consult your physician and physical therapist for a program designed specifically for your needs.
The anatomical and physiological changes in the body associated with age must be respected and considered when establishing an exercise program for those over 50. One common change that occurs with age is the loss of the density and quality of bone and cartilage. In addition to loss of bone density, especially in women, osteoarthritis destroys the cartilage in the joints and reduces the space between the bones in a joint. For example, a loss of space in the shoulder joint makes it more likely to impinge the structures that pass through the joint such as the bursa and rotator cuff tendons. Overtime, the impingement will lead to small tears, then bigger tears and possibly a full tear. This can be avoided by modifying the exercises and activities performed at the shoulder. The degenerative knee joint is another example of a how the degenerative and arthritic process creates a narrow space which leads to further damage if modifications in exercise and activities are not modified. When the knee degenerates, it often begins by a dehydration and degeneration of the cartilage at the end of the bones and between the joint of the knees. Certain activities and exercises will accelerate this process. Running and jumping are two of these activities but squatting, especially deep knee bends with heavy weight on the shoulders or in the hands, can be equally damaging. Muscles and tendons are at risk in the aging body as well. As these tissues degenerate and lose their elasticity, they are very susceptible to pulls and tears, especially when not properly warmed-up and stretched. The best examples of an aged and degenerative tendon leading to a more serious problem when not warmed up and stretched properly is an Achilles tendonitis (often caused by overuse or running hills) or Achilles tendon tear (often caused by a sudden burst and stretch such as reaching for a shot in tennis or racquetball).
Shoulder Dips
The shoulder joint was not meant to bear weight through its full range of motion. Lowering the entire weight of the body on the shoulder places excessive compression through the joint, can lead to rotator cuff impingement and tears as well as tearing of the labrum. (Photo 6: Shoulder Dips – through the full range of motion – Not Recommended). A plank is one alternative to this exercise. Also, this exercise works the triceps and latissumus dorsi (lat) muscles. A second and more practical alternative would be to exercise the muscles separately. For example, the triceps are best performed while lying on your back as described above. (See Photo 3 in Part 1) and the lats can be better worked with pulleys or bands performing a row or sawing motion. (PHOTO 7: Standing Lats with Exercise Bands - Recommended).

Deep Squats
WATCH THE KNEES! Squats work the quads and the gluts but a full squat can be very damaging to the knees. (Photo 8: Deep Squat – through the full range of motion – Not Recommended). Instead, work the quads while on a knee extension machine and work the gluts while extending the hip in standing. A partial squat is acceptable, as you lower the body to 30 or 45 degrees. The squat can be advanced with 5-10 dumbells in your hands, not overhead. (PHOTO 9: Half Squat with Dumbells - Recommended).


Full Sit-Ups
Full sit-ups are bad for your back and exercise the muscles of the hip more than those of the abdomen. (Photo 10: Full Sit-up – Not Recommended). A better sequence is to begin using the legs for resistance to the lower abs and advance to a partial sit up or curl. (PHOTO 11: Half Squat Sit-up or Curl - Recommended).

Gravity Assisted Inverted Traction
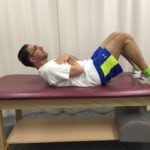
The blood vessels of the brain were not intended to work against gravity with the head upside down. As a result, blood and pressure build up in the cranium. Consequently, there are documented cases of people having a stroke during inverted traction due to a weakness in a blood vessel in the brain. There are safer and effective forms of traction/decompression according to the research such as hook lying with your legs on chair. (PHOTO 12: Hook Lying on Chair for Lumbar Decompression – Recommended) Another alternative is to have someone pull your legs while lying on your back with your knees bend and resting on a bolster or a few pillows. (PHOTO 13: Manual Traction for Lumbar Decompression – Recommended)


Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Visit your doctor regularly and listen to your body.
Part 1 of 2: SAVE YOUR JOINTS! Exercises You Should Avoid if You’re Over 50!
Why Change is Necessary with Age…
For many years, I have repeatedly preached about the value of engaging in an active lifestyle throughout life. It is especially important to be active as one gets older in order to maintain mobility and independence. However, many take this advice to an extreme and refuse to accept the inevitable changes that occur in the body with age. They run, jump, lift and throw like a teenager and often fail to modify their activity or exercise regimen appropriately for their age. Consequently, they suffer from multiple injuries, including muscle tears, tendonitis, bursitis, impingement and advanced osteoarthritis. Keep in mind, everyone ages differently. One person at 60 years of age may be the equivalent of another at 50. However, change with age is inevitable, so be kind to your body…it’s the only one you have! It is always prudent to consult your physician and physical therapist for a program designed specifically for your needs.
The anatomical and physiological changes in the body associated with age must be respected and considered when establishing an exercise program for those over 50. One common change that occurs with age is the loss of the density and quality of bone and cartilage. In addition to loss of bone density, especially in women, osteoarthritis destroys the cartilage in the joints and reduces the space between the bones in a joint. For example, a loss of space in the shoulder joint makes it more likely to impinge the structures that pass through the joint such as the bursa and rotator cuff tendons. Overtime, the impingement will lead to small tears, then bigger tears and possibly a full tear. This can be avoided by modifying the exercises and activities performed at the shoulder. The degenerative knee joint is another example of a how the degenerative and arthritic process creates a narrow space which leads to further damage if modifications in exercise and activities are not modified. When the knee degenerates, it often begins by a dehydration and degeneration of the cartilage at the end of the bones and between the joint of the knees. Certain activities and exercises will accelerate this process. Running and jumping are two of these activities but squatting, especially deep knee bends with heavy weight on the shoulders or in the hands, can be equally damaging. Muscles and tendons are at risk in the aging body as well. As these tissues degenerate and lose their elasticity, they are very susceptible to pulls and tears, especially when not properly warmed-up and stretched. The best examples of an aged and degenerative tendon leading to a more serious problem when not warmed up and stretched properly is an Achilles tendonitis (often caused by overuse or running hills) or Achilles tendon tear (often caused by a sudden burst and stretch such as reaching for a shot in tennis or racquetball).
Always warm up for 5 to 10 minutes before exercise (run in place, slow jog, pedal a bike slowly), then stretch slowly, gently and pain free. Gradually warm into aerobic exercise and begin weight training with light weights, gradually increasing to heavier. Following exercise, perform stretching or yoga. Remember, low weights with high repetitions are safer for those over 50. Also, dumbbells are more comfortable and safer because they allow one to modify the grip and position of the arm easier than a barbell.
Some high impact aerobics are worse than others. Running, for example, has been shown to transmit 3 times the body weight of the runner to the joints of the lower body. Running, jumping, (jumping rope), step aerobics, impact plyometrics (box jumps) and impact calisthenics (jumping jacks) are the best examples of high impact aerobics that can accelerate wear and tear to your joints.
With this in mind, those over 50 would be well-advised to engage in low-impact aerobics on a regular basis. For example, if you want to run two to three days per week, do not run two days in a row and consider performing low impact exercise in between. Some examples of low impact aerobics are: walking, treadmill walking, swimming, elliptical trainer, and an exercise or road bike.
Military press and overhead triceps are two examples of lifting weight overhead that are potentially harmful for several reasons: One, lifting a weight overhead hyperextends and compresses the spine, putting it at risk for advanced osteoarthritis and degenerative disc disease, especially in those over 50. Two, when the shoulder lifts weight overhead, the rotator cuff and bursa can be impinged in the shoulder joint space, especially in those over 50 with a narrower space. Overtime, this may lead to impingement syndrome, bursitis, chronic tendonitis, and rotator cuff tears. (PHOTO 1: Overhead Press – Not Recommended)
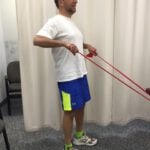
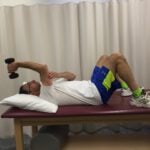
Better Alternative: Instead of lifting overhead to strengthen the deltoid and triceps (muscles used in military press), consider a 70 degree lateral raise with low to moderate weight and higher repetitions. (PHOTO 2: Lateral Shoulder Raise 45-75 degrees – Recommended Alternative). To work the triceps, lying on your back with a dumbbell in one hand, extend your elbow to contract the triceps. Use the opposite hand to support the back of the elbow during the exercise. (PHOTO 3: Triceps - while lying on your back - Recommended Alternative).


A bench press through a full range of motion, which fully extends the arms then lowers the weight to the chest, hyperextends the shoulder and puts the internal structures of the shoulder joint at risk. It is a common position to tear the anterior capsule, rotator cuff or labrum of the shoulder, especially in the tight and dehydrated shoulder tissues of those over 50. (Photo 4: Bench Press – through the full range of motion – Not Recommended). As a safer alternative, consider using a 6-8 inch block on the chest to limit the extent to which the shoulder is hyperextended as the bar will be blocked before it touches the shoulder. A second and more practical alternative would be to use dumbbells while lying on the floor. The dumbbells will allow for more comfortable and safer arm position as opposed to a barbell and the floor will block the arms from hyperextending beyond a safe range. (Photo 5: Safe Bench Press – using hand-held dumbbells on the floor with limited range of motion – Recommended).


Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” in the Scranton Times-Tribune. Next week: Part 2 “Exercises to Avoid if You’re Over 50!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Dr. Kafrissen
MAY IS MENTAL HEALTH MONTH! Exercise and Be Happy!
TCMC Medical Contributor: Steven Kafrissen, MD, is a psychiatrist at Community Counseling Services and an associate professor of clinical medicine at The Commonwealth Medical College.
This column is a special feature the third Monday of every month of Health & Exercise Forum in cooperation with The Commonwealth Medical College.
Living in a region of the country that has a 50-percent chance of sunshine is not for the faint at heart! It can certainly affect one’s mood. However, there is something you can do about it…exercise! Studies show that one of the most understated benefits of exercise is mental health. Specifically, exercise that is aerobic (exercise that increases your heart rate for 30 minutes or more), such as walking, biking, running, swimming, hiking or using an elliptical or stepper machines to name a few, is the secret to the “runner’s high.” This exercise euphoria is not limited to runners alone, but all who engage in aerobic exercise are more likely to experience high energy, positive attitude and mental wellness.
Physical activity, specifically aerobic exercise, is a scientifically proven, useful tool for preventing and easing depression symptoms. Studies in the British Journal of Medicine and the Journal of Exercise and Sports Science found that depression scores were significantly reduced in groups that engaged in aerobic running, jogging or walking programs, 30-45 minutes three to five days per week for 10 to 12 weeks, when compared to a control group and a psychotherapy counseling group.
Depression is the most common mental disorder and is twice as common among women as in men. Symptoms include: fatigue, sleeplessness, decreased appetite, decreased sexual interest, weight change and constipation. Many of these symptoms are likely to bring an individual to his or her family physician. Unfortunately, depression is on the increase in the United States. According to the National Ambulatory Medical Care Survey, in the 1990s, 7 million visits to a primary care physician were for the treatment of depression. Ten years later, the number doubled.
In addition to exercise, patients and their loved ones should remember they can call Helpline (888-829-1341 or 570-829-1341 or text your zip code to 898211) or a crisis service for any suicidal ideas (570-348-6100 in Lackawanna County and 570-552-6000 in Luzerne). Also, be aware that mental health centers are available (Scranton Counseling Center, Community Counseling Center, Northeast Counseling Services and other community and private mental-health providers).
According to medical literature, exercise reduces depression in two ways, psychologically (mentally) and physiological (physically).
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Read “Health & Exercise Forum” by Dr. Mackarey every Monday in the Scranton Times-Tribune.
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College
