 ARTHRITIS OF ANKLE
ARTHRITIS OF ANKLE
I have been advising my patients to exercise, keep active, and walk as long as they can in order to stay mobile and healthy. However, seniors and others suffering from repeated trauma such as fractures and sprains, often tell me activities that require prolonged walking is limited by ankle pain from arthritis. They often ask, “What is arthritis of the ankle?” How does it happen? What can I do about it?
Gerry Davis, assistant baseball coach at Lackawanna College, is a typical example of the ankle arthritis journey. He has suffered for many years from ankle arthritis and pain. He sustained repeated injuries as a young athlete and, when conservative treatment was no longer effective and he was no longer able to walk without a painful limp, he had an ankle replacement.
Your family physician will examine your ankle to determine if you have arthritis. In more advanced cases you may be referred to a specialist such as a podiatrist, orthopedic surgeon or rheumatologist for further examination and treatment. X-rays will show if the joint space between the bones in the ankle is getting narrow from wear and tear arthritis. If rheumatoid arthritis (RA) is suspected, blood tests and an MRI may be ordered. The diagnosis will determine if your problem is minor, moderate or severe.
In the early stages your treatment will be a conservative, nonsurgical approach, which may include; anti-inflammatory medication, orthopedic physical therapy, exercise, activity modifications, supplements, bracing, etc. You and your family physician, podiatrist, orthopedic surgeon or rheumatologist will decide which choices are best.
Visit your doctor regularly and listen to your body.
EVERY MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Mario Cornacchione, D.O.
TCMC Author: Dr. Mario Cornacchione DO
Dr. Cornacchione, a specialist in Geriatric Medicine, is an Associate Professor and Assistant Chair of Family Medicine in the Department of Clinical Sciences at the Commonwealth Medical College. He is also the Research Director at the Northeastern Pennsylvania Memory and Alzheimer’s Center where he currently is the principal investigator in clinical trials studying new disease modifying agents for the treatment of Alzheimer’s disease and prodromal Alzheimer’s disease (MCI).
Dr. Cornacchione is a national speaker on a wide range of topics on geriatric medicine, dementia, aging and long term care. He is a coauthor and reviewer of a number of National Clinical Practice Guidelines in long term care and on the editorial board of the Journal of Parkinson and Alzheimer’s Disease.
WORLD ALZHEIMER’S AWARENESS MONTH
September is World Alzheimer's Awareness Month. It would be very unusual to find a person whose life has not been affected by someone with Alzheimer’s disease (AD). Unfortunately, there is a tsunami coming of those baby boomers that will develop the disease. AD is only one form of dementia and an estimated 5.4 million Americans of all ages currently have the disease.
The future numbers are even more staggering:
Although older age is a risk factor, Alzheimer’s is not a normal part of aging, and older age alone is not sufficient to cause the disease. A family history of Alzheimer’s is not necessary for an individual to develop the disease. However, individuals who have a parent (especially a mother), brother or sister with Alzheimer’s are more likely to develop the disease than those who do not have a first-degree relative with AD.
Alzheimer’s disease symptoms vary among individuals. The most common initial symptom is a gradually worsening ability to remember new information. This occurs because the first neurons to be damaged and destroyed are usually in brain regions involved in forming new memories. As neurons in other parts of the brain are damaged and destroyed, individuals experience other difficulties. The following are common symptoms of Alzheimer’s:
As a geriatrician who has taken care of thousands of pateients with Alzheimer’s I can tell you this disease not only eventually steals the essence of who a person is and what their life has been, but also inflicts a large toll on the families of those affected.
No single, simple test exists to diagnose Alzheimer’s disease. Although physicians can almost always determine if a person has dementia, it may be difficult at times to identify the exact type of dementia. We use a variety of approaches and tools to help make a diagnosis. They include the following:
Not all memory issues are due to a dementia such as AD. Mild Cognitive Impairment (MCI ) is a condition in which an individual has mild but measurable changes in thinking abilities that are noticeable to the person affected and to family members and friends, but do not affect the individual’s ability to carry out everyday activities. Approximately 15 percent to 20 percent of people age 65 or older have MCI. People with MCI, especially MCI involving memory problems, are more likely to develop Alzheimer’s and other dementias than people without MCI. A recent systematic review of 32 studies found that an average of 32 percent of individuals with MCI developed Alzheimer’s disease in 5 years.
There is sufficiently strong evidence that regular physical activity and management of cardiovascular risk factors (especially diabetes, obesity, smoking and hypertension) reduce the risk of cognitive decline and may reduce the risk of dementia. In addition, a healthy diet and lifelong learning/cognitive training may reduce the risk of cognitive decline.
Thing that may lower your risk of developing Alzheimer’s disease:
Alzheimer’s disease is and will continue to be the major health crisis for the US to deal with in this century. With nearly 14 million people who will have the disease by 2050 it is essential that people with AD and those with mild cognitive impairment participate in clinical trials to help find a medication which will prevent, reverse, delay the onset of or significantly slow the course of the disease. We are fortunate to have clinical trials of potential new medications available locally at the NEPA Memory and Alzheimer’s Center in Plains, PA.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
ACL INJURY PREVENTION FOR FEMALE ATHLETES: Part 2 of 2

Danielle Maurice, SPT
Guest Contributor: Danielle Maurice, SPT
Various studies have shown that female athletes are on average four times more likely than males to tear their anterior cruciate ligament (ACL) of the knee. Susceptibility for female athletes to an ACL injury is a multifaceted problem; anatomical, mechanical, physiological factors and landing technique are all involved. Studies done involving the Prevent Injury and Enhance Performance (PEP) program developed by the Santa Monica Sports Medicine Research Foundation has demonstrated a decrease in ACL injuries for those athletes that adopted the program, compared to those that did not engage in a prevention program. Usually, athletes first get exposed to such programs once they get to the college level, mostly being applied at the Division I level. As the coach of the Pocono Snow Junior’s U13 Girls Team and as an Pre- Physical Therapy/Exercise Science student at the University of Scranton, I have become very interested in applying an injury prevention program to the regular practice routine for the girls I coach sooner than the collegiate level. With the help of Dr. Paul Mackarey and University of Scranton Assistant Coach Sarah Jerome, we created an ACL prevention program, based off of the PEP program, to tend to the needs of these girls. Last week we discussed the anatomy and mechanism of the ACL injuries in female athletes and the prevention program weeks 1 and 2. This week we will continue with the ACL prevention program for weeks 3-4 and 5-6.
Weeks 3-4
As in Weeks 1 and 2, start with one lap around the field, followed by the dynamic warm up and hops. New to Weeks 3 and 4 are agility exercises. Agility exercises can be modified to be sport specific. With the intent of increasing balance and strength for the athletes, proper body positioning and landing techniques are important here. A good sport specific agility exercise is Figure 8’s (Photo 13—Figure 8’s), or use of an agility ladder (Photo 14).
Weeks 5-6
The last two weeks of the program begin with the warmup lap around the field and the dynamic warmup (the same as Weeks 1-4). Here, it is the coach’s choice for either hops or agility/ladder work. New to Weeks 5 and 6 are advanced plyometrics and resistance exercises.
Reminder: Plyometrics are meant to be explosive and build strength, speed, and power. However, technique is still important! Remind athletes to land softly on the balls of their feet with bent knees—never landing on heels or hyperextended knees.
Examples of advanced plyometric exercises include: Jump squats (Photo 15), knee-to-chest (Photo 16), single leg lateral hops (Photo 17), and mountain climbers (Photo 18). These exercises should be done for 10 yards, then athletes should accelerate for another 10 yards.
A great resistance exercise is sports cord with a partner (Photo 19). By having one athlete running forward while attached to a band, and another athlete holding it behind them, both athletes are working on improving strength and balance.







CONCLUSION:
For several reasons, including anatomy and bio mechanics, female athletes have four times the risk of ACL injuries. Studies have shown that a multifaceted ACL injury prevention program can significantly reduce the risk for an ACL injury in this population. A multifaceted program includes education in anatomy, biomechanics, and physiology, along with concentration on lower extremity strength, flexibility, agility, balance and proprioception with emphasis on proper landing techniques.
Coaches, athletic trainers, athletic directors, school boards, parents and players would be well advised to incorporate a mandatory ACL injury prevention program such as the one described in part I and II of this column in order to prevent ACL injuries in all athletes, most especially the female athlete.
Guest Contributor: Danielle Maurice, SPT, University of Scranton, Pre- Doctor of Physical Therapy/Exercise Science Student 2020. Dani a native of Long Island, NY is an intern at Mackarey & Mackarey Physical Therapy Consultants, LCC
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Danielle Maurice, SPT
ACL INJURY PREVENTION FOR FEMALE ATHLETES: Part 1 of 2
Guest Contributor: Danielle Maurice, SPT
Various studies have shown that female athletes are on average four times more likely than males to tear their anterior cruciate ligament (ACL) of the knee. Susceptibility for female athletes to an ACL injury is a multifaceted problem; anatomical, mechanical, physiological factors and landing technique are all involved. Studies done involving the Prevent Injury and Enhance Performance (PEP) program developed by the Santa Monica Sports Medicine Research Foundation has demonstrated a decrease in ACL injuries for those athletes that adopted the program, compared to those that did not engage in a prevention program. Usually, athletes first get exposed to such programs once they get to the college level, mostly being applied at the Division I level. As the coach of the Pocono Snow Junior’s U13 Girls Team and as an Pre-Physical Therapy/Exercise Science student at the University of Scranton, I have become very interested in applying an injury prevention program to the regular practice routine for the girls I coach sooner than the collegiate level. With the help of Dr. Paul Mackarey and University of Scranton Assistant Coach Sarah Jerome, we created an ACL prevention program, based off of the PEP program, to tend to the needs of these girls. Before getting into the program itself, here is some background information about the function of the ACL and why strengthening and retraining the surrounding muscles are important.
What is the ACL?
ACL stands for anterior cruciate ligament and it prevents anterior translation (forward movement of the femur/thigh bone from the tibia/shin bone) The ACL also acts to stabilize the knee joint and prevent hyperextension (Photo 2—Normal knee vs. Hyperextended knee)
How is it injured in female athletes?
70% of ACL injures are non-contact injuries, most commonly occurring during landing or sharp decelerations. Females are more prone to these injuries due to anatomical and physiological differences compared to males. Females have wider hips, resulting in “knocked-knees” (Photo 3—Normal knee vs. knocked-knees) and hyperextension of the knee. In addition, the hormone estrogen causes greater laxity in ligaments. Also, females have greater hamstring flexibility than males, allowing more anterior translation. Being more vulnerable to hyperextension as a result of these factors places more stress on the knee joint and the ACL, leaving females more susceptible to injury.
How do we prevent ACL injuries?
There are five essential components to a good ACL prevention program. They include:
The ACL prevention program we created includes all five of these components. This program is intended to be completed two times per week, in a six week cycle. Below, the program has been broken up into weekly sessions, with a new element added after two weeks.
Weeks 1-2
The dynamic warm up is done to help increase flexibility for the athletes. Contrary to popular opinion, dynamic stretching is better for athletes when compared to static stretching. Dynamic stretching involves continuous movement while stretching, opposed to static stretching where athletes are stationary. Dynamic stretching is more beneficial as it helps increase range of motion and flexibility, which will ultimately reduce risk of injury and improve performance.
Although hops may seem like a simple exercise, they actually help encourage proper technique, while strengthening leg muscles and improving balance. To start, hops should be done over a line on the field, eventually progressing to jumping over cones or hurdles. While engaging in the exercise, coaches should make sure athletes are not locking out their knees and are maintaining proper body alignment (Photo 12—Two Legged Hops). Different hopping exercises include:











NEXT WEEK: In Part 2 of 2 on ACL Prevention will present Weeks 3-4 and Weeks 5-6 of the Program.
Guest Contributor: Danielle Maurice, SPT, University of Scranton, Exercise Science/Pre-Doctor of Physical Therapy Student 2020, a native of Long Island, NY is a student physical therapy aide at Mackarey & Mackarey Physical Therapy Consultants, LCC
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Part II of II ACL Prevention. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Victoria Wrightson, SPT
Concussions in Football: Part 2 of 2
Guest Contributor: Victoria Wrightson, SPT
There is a heightened awareness of concussions in football due to the recent discovery of a degenerative brain disease found during the autopsies of professional football players now known as chronic traumatic encephalopathy, or CTE. The Mayo Clinic defines CTE as brain degeneration caused by repeated head trauma. Symptoms include difficulty thinking, impulsive behavior, depression, emotional instability, and substance abuse, to name a few, but the full list of symptoms remains unknown. With football season quickly approaching, it is important for coaches and parents to consider the safety of their players while at practice and during competition. Although the topic of concussion isn’t new, I think it is important to remind readers of what a concussion are the potential long-term effects of concussion, and what actions can be taken to keep athletes safe. Last week, in “Concussion Part 1” we discussed the symptoms and classification of concussions. This week we will discuss prevention of concussions in football.
Given the serious potential consequences of concussions and head impact, actions should be taken to prevent them (Table 1 Prevention of Concussion). Advances in technology are leading to better and safer helmet designs. Earlier this year, a Seattle-based company, VICIS, released a state-of-the-art helmet designed to better absorb head impact forces. This model, the ZERO1, differs from standard helmets in a few key ways. First, the outer shell of the ZERO1 is not hard, but rather a flexible plastic that slightly gives upon impact, then returns to its original form. Second, the ZERO1 helmet’s core is layered in columns, designed to slow forces that come from any direction. Finally, the inner shell of the helmet is made of memory foam, which forms to each player’s unique head shape. These revolutionary helmets will be tested this year by the University of Washington Huskies.
Actions can also be taken by coaches and players without having to spend money on high-tech helmets. Proper tackling technique should be taught by coaches, especially in young athletes. Emphasis should be placed on tackling with the shoulders, rather than head-first.
Studies have shown that strengthening the neck muscles may reduce player’s risk of head injury. Researchers at the Colorado School of Public Health and Nationwide Children’s Hospital found that neck strength predicts concussion risk regardless of the athlete’s gender or sport. They found that players with the weakest neck muscles suffered from the greatest number of concussions. Strong neck muscles can help slow the acceleration of the head during impact, and therefore lower the risk of traumatic brain injury. Exercises that target the neck muscles can easily be incorporated into practice. (Table 2 – Isometric Neck Strengthening Exercises).
In addition to technology, tackling technique, and neck strengthening, there is one more important action that needs to be taken in order to prevent concussion in football- limiting the amount of contact during practice. Research demonstrates that limiting full-contact practices reduces the number of concussions in football. For example, in 2012 the NFL placed limits on the number of full-contact practices. That year, the number of concussions during practices declined. Recently, the Division I Ivy League Conference football coaches made an executive decision: full-contact hitting practices will not be permitted during the regular season. In a recent article in Bleacher Report, Adam Kramer wrote a very compelling and informative piece entitled, “The Future of Football Practice – What a “no – tackle practice” looks, feels and sounds like.” In his article he describes the techniques developed by Dartmouth football coach Buddy Teevens, as he turned the team around from 0-10 season to Ivy League Champions utilizing a “no-tackle practice” approach. The team uses a “Mobile Virtual Player” (MVP) designed by Elliot Kastner, a Dartmouth engineering student and former football player. The virtual tackling dummy is controlled remotely by the coach to simulate and actual player. The team reduced their missed tackle rate by more than 50%. For more information, view the video, “The Dartmouth Way,” on YouTube.
THE BURNING QUESTION: If NCAA teams can do it, why can’t youth and high school football teams follow this example?
In conclusion, concussions are not only a serious problem in the short term, but they can also lead to adverse long-term consequences. With research showing that repetitive head trauma poses significant risk, one needs to take action to prevent concussions from happening. Coaches, athletic trainers, athletic directors, school boards, parents and players would be well advised to incorporate a mandatory concussion prevention program such as the one described in part I and II of this column in order to prevent concussions in all athletes, especially football players. Prevention includes; purchasing proper equipment, teaching proper tackling techniques, implementing adequate fitness programs such as neck strengthening exercises and limiting full-contact sessions such as the program adopted by the College Football Division I Ivy League Conference. Let us begin the discussion on this important topic to raise the level of awareness toward change …you may be saving someone’s future!
Table 1: Prevention of Concussions
Table 2: Isometric Neck Strengthening Exercises





Guest Contributor: Victoria Wrightson, SPT, Temple University, Doctor of Physical Therapy Student 2018. Victoria, a native of Scranton, PA, is an intern at Mackarey & Mackarey Physical Therapy Consultants, LLC.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
CONCUSSIONS IN FOOTBALL: Part 1 of 2
Victoria Wrightson, SPT
Guest Contributor: Victoria Wrightson, SPT
Football fan or not, you have probably heard of the 2015 movie, Concussion, that caused somewhat of a headache (no pun intended) for the NFL. Based on a true story, the movie highlights the discovery of a degenerative brain disease found during the autopsies of professional football players now known as chronic traumatic encephalopathy, or CTE. The Mayo Clinic defines CTE as brain degeneration caused by repeated head trauma. Symptoms include difficulty thinking, impulsive behavior, depression, emotional instability, and substance abuse, to name a few, but the full list of symptoms remains unknown. As a student physical therapist, I learn a great deal about the anatomy of the brain and serious consequences of brain injury. As an avid football fan, I have great interest in the treatment, rehabilitation, and more importantly, the prevention of sports injuries. With football season quickly approaching, it is important for coaches and parents to consider the safety of their players while at practice and during competition. Although the topic of concussion isn’t new, I think it is important to remind readers of what a concussion are the potential long-term effects of concussion, and what actions can be taken to keep athletes safe.
“Traumatic brain injury.” Sounds scary, right? In fact, this is exactly what a concussion is - the most common form of brain injury. Concussions are caused by blows to the head or by hits to the body that cause the brain to move around, forcefully bumping the skull’s inner walls. This leads to altered brain function and to symptoms that may not be immediately obvious. While symptoms typically appear soon after the injury, some may not become apparent for hours or days later. Common signs and symptoms of concussion include:
Concussions are graded based upon severity. Researchers in sports medicine have developed a system to grade concussions based upon loss of consciousness, post-traumatic amnesia, and symptoms such as the ones mentioned above. This system, known as the McGill concussion grading system, is described in Table A.
Just how common are head injuries in football? According to researchers at the University of Rochester, repetitive head impacts in a single football season range from 244 to 1,944 impacts per player. According to the 2015 NFL Injury Report, 271 concussions were diagnosed during preseason and regular-season practices and games combined. With the high rates of head impact in football, it is important to realize what long term effects may result.
Concussions may lead to serious long-term consequences, and even worse effects may be seen in those who suffer from more than one. Studies have indicated that deficits in memory, attention, and concentration can be seen long after the time of initial injury. One study found that measures of attention and concentration were significantly worse in high school athletes who had suffered from a concussion in the past. This study also found that high school athletes with a history of concussion had a significantly lower GPA than their peers. As previously mentioned, repetitive head trauma can lead to a serious condition known as chronic traumatic encephalopathy (CTE).
Next week, in “Concussion Part 2” we will discuss prevention of concussions in football.
TABLE A: McGill Concussion Grading System
| GRADE | Characteristics |
| 1 | No loss of consciousness, no post-traumatic amnesia |
| 1A | No post-concussion symptoms, only seconds of confusion |
| 1B | Post-concussion symptoms and/or confusion that resolved in 15 min |
| 1C | Post-concussion symptoms and/or confusion that does not resolve in 15 min |
| 2 | Post-traumatic amnesia for less than 30 min. and/or loss of consciousness for less than 5 min. |
| 3 | Post-traumatic amnesia for more than 30 min. and/or loss of consciousness for more than 5 min. |
Source: Leclerc S, Lassonde M, Delaney JS, Lacroix VJ, Johnston KM. Recommendations for grading of concussion in athletes. Sports Medicine. 2001;31(8):629-636. doi:10.2165/00007256-200131080-00007.
Guest Contributor: Victoria Wrightson, SPT, Temple University, Doctor of Physical Therapy Student 2018. Victoria a native of Scranton, PA is an intern at Mackarey & Mackarey Physical Therapy Consultants, LCC
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune: Concussions Part 2 of 2. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.

Kathryn Swatkowski, CNM
TCMC Guest Author: Kathryn N Swatkowski, CNM
TCMC Medical Guest Author: Kathryn N. Swatkowski, CNM has been a Certified Nurse Midwife for 20 years, taking care of women throughout their life-span from adolescence through menopause. She is a clinical instructor of obstetrics and gynecology at The Commonwealth Medical College.
This column is a special feature the third Monday of every month of Health & Exercise Forum in cooperation with The Commonwealth Medical College.
August is National Breastfeeding Awareness Month
Expectant mothers typically do all they can to ensure their baby’s health. A wholesome diet, regular exercise and avoiding harmful habits like smoking are all important things a woman should do during pregnancy. However, there is something additional mothers can do AFTER their child’s birth that can be equally, if not more, important and has been around as long as human life itself… breastfeed! While far from new, it is has been rediscovered for it tremendous benefits and gaining popularity.
Breastfeeding has innumerable benefits for mother and child. For example, nursing your baby right after birth helps solidify the bond between you and your baby. Moreover, the health benefits to baby begin right away. That’s because your breasts produce colostrum beginning during pregnancy and continuing through the early days of breastfeeding. Colostrum precedes breast milk and has plenty of antibodies to help keep your baby healthy. Colostrum is extremely easy to digest, and is therefore the perfect first food for your baby. Also, as the La Leche League (LLL) tells new mothers, “Colostrum has a laxative effect on the baby, helping him pass his early stools, which aids in the excretion of excess bilirubin and helps prevent jaundice.” Jaundice is common in newborns and is usually treated by placing the baby under special lights. LLL also points out that the concentration of immune factors is much higher in colostrum than in mature milk, which comes in after about two weeks.
The positive effects continue for both mother and baby as the child grows from newborn to infant. Breast-fed babies are, for example, are less prone to sudden infant death syndrome (SIDS), an unexplained death of a healthy infant while sleeping. The peak incidence of SIDS occurs when a baby is about three months old. It is an unspeakable tragedy that affects entire families. While we must be very clear that breastfeeding is not a guarantee against SIDS, newer studies have shown that infants who were never breastfed may have two to three times the risk of dying of SIDS. Although the actual mechanism is unknown, some theories are that breastfeeding may provide defense against SIDS because it lowers a baby’s risk of infection through antibodies passed on by mom or because human milk is ideally equipped to nurture human brains -- and the brain controls sleep cycles.
Additional Benefits for Baby:
Additional Benefits for Mom:
Are there ever reasons why either mother or baby should not breastfeed? While extremely unusual, there are contraindications for breastfeeding. Mothers who must take certain medicines may be unable to nurse. There are also some conditions in newborns – some treatable – that may limit or prevent breastfeeding. Your physician (obstetrician/gynecologist or pediatrician) or midwife should be consulted before you take any medications, vitamins or herbals.
Finally, new parents are frequently worried about their breast-fed babies because they can’t “see” how much nutrition their child is getting. A good rule of thumb is that a breast-fed baby will have a wet or dirty diaper as many times a day as he or she is days old. For example, one wet/dirty diaper the first day of life, two the second, and so forth for about a week. After that first week, look for six to eight wet diapers daily and a bowel movement about once a day.
It is recommended that you exclusively breastfeed your baby for the first six months and continue for at least the first year. After that, it’s up to you. It’s also important to know that every baby is a unique individual. Don’t become alarmed if your child doesn’t seem to adhere to what the textbooks say. Instead, turn for support to some reliable and trustworthy: your physician, midwife and the La Leche League.
SOURCE: Le Leche League is an international nonprofit organization that distributes information on and promotes breastfeeding. www.lllusa.org
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquiries related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 3 of 3
When the shoulder is compromised by loss of motion or strength, so too is the function of the arm and hand. It becomes difficult to dress, groom, work, play sports, etc. Therefore, it is imperative that we maintain shoulder health through range of motion and strength exercises. However, it is equally important that we exercise in a manner that does not compromise the integrity of shoulder motion or strength. With this in mind, this column will present a list of specific exercises to maintain or regain shoulder strength without compromising the joint and muscles.
Shoulder Strengthening Exercises
Dynamic – Isometric Exercises – by moving the body – not the shoulder. These exercises offer a very unique way to safely strengthen the shoulder as originally designed by Dr. Gary Mattingly.
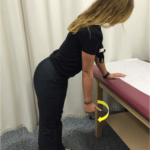
To perform these exercises, tie a resistance band to a post or a door knob, at waist level. Begin using the lowest tension band (yellow). Please note, however, that a red resistance band is used in the photos for enhanced visibility. The exercise is to be performed slowly and repeated 5 times. After one or two weeks, the repetitions may be increased to 8 or 10 times. Also, begin with exercises A, B and C the first week or two. If no problems arise, then proceed with exercises D, E and F.
Shoulder Extension – PHOTO A: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder, elbow and wrist locked. Facing the post where the band is tied, slowly take up the slack in the band. Slowly walk backwards 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk forwards toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.
Shoulder Adduction – PHOTO B: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder, elbow and wrist locked. Position your body with your right shoulder pointing to the post where the band is tied; slowly take up the slack in the band. Slowly walk sideways toward the left 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk sideways to the right toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.
Shoulder Internal Rotation – PHOTO C: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder and wrist locked with your elbow bent at 90 degrees. Position your body with your right shoulder pointing to the post where the band is tied; slowly take up the slack in the band. Slowly walk sideways toward the left 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk sideways to the right toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.
Shoulder Flexion – PHOTO D: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder, elbow and wrist locked. Position your body with your back toward the post where the band is tied; slowly take up the slack in the band. Slowly walk forwards 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk backwards toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.
Shoulder Abduction – PHOTO E: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder, elbow and wrist locked. Position your body with your left shoulder pointing to the post where the band is tied; slowly take up the slack in the band. Slowly walk sideways toward the right 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk sideways to the left toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.
Shoulder External Rotation – PHOTO F: Place a yellow resistance band in your right hand. Stand up straight and keep your shoulder and wrist locked with your elbow bent at 90 degrees. Position your body with your left shoulder pointing to the post where the band is tied; slowly take up the slack in the band. Slowly walk sideways toward the right 5 or more steps until tension is felt in the arm and hold this position for 5 seconds. Then, slowly walk sideways to the left toward the post until tension in the band is released. Repeat 5 times. Then, repeat on the left side.






Contributions: Gary Mattingly, PT, PhD, Professor Emeritus, University of Scranton, Physical Therapy Department.
Read Dr. Mackarey’s Health & Exercise Forum – every Monday.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 2 of 3
The shoulder, working as a ball and socket, is most flexible joint in the human body. It is comprised of two separate joints, the union between the glenoid fossa, (the socket at the end of the scapula or shoulder blade, and the ball at the end top of the humerus, or upper arm bone. The second articulation at the shoulder involves the acromioclavicular joint that connects your scapula to your collar bone. While it is held together by various ligaments, the muscles of the shoulder, namely the rotator cuff, generate the force that allows it to move in multiple directions. The flexibility of the shoulder is thought to be an evolutional advancement as it permits the upper arm to place the hand, and more importantly, the opposing thumbs, in uncountable positions, allowing humans to function at a higher level than other mammals. The ability to paint, draw, play musical instruments, cook, clean, be creative, build, cultivate food, etc. are all directly related to the beautiful and complex cooperative effort between the shoulder, arm and hand.
When the shoulder is compromised by loss of motion or strength, so too is the function of the arm and hand. It becomes difficult to dress, groom, work, play sports, etc. Therefore, it is imperative that we maintain shoulder health through range of motion and strength exercises. However, it is equally important that we exercise in a manner that does not compromise the integrity of shoulder motion or strength. With this in mind, this series of 3 columns will present exercises to maintain or regain shoulder range of motion without compromising the joint and muscles.
Shoulder Range of Motion Exercises
Always perform slowly and without pain. Perform 5 to 10 repetitions and repeat on the opposite side.
Pendulums – PHOTO 1: Stand facing a table or counter top. Lean over and allow your arm to hang down like a pendulum. Turn your thumb up pointing to 12:00. Slowly swing your arm clockwise in 6 to 12 inch circles. Perform 5 times and repeat counter-clockwise.
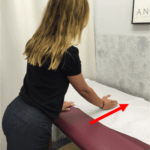
Table Slides – PHOTO 2: Stand facing a table or counter top. Lean over and allow your arm to rest on the table. Turn your thumb up pointing to 12:00. Slowly slide your arm forward to stretch the shoulder. H4:old 5 seconds. Perform 5 times.
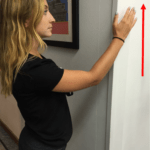
Wall Slides – PHOTO 3: Stand in a door way and face the wall of the door jam. Turn your thumb up pointing to 12:00. Slowly slide your hand/arm up the wall to stretch the shoulder. Hold 5 seconds. Perform 5 times.
Touch Ear/Back of Head – PHOTO 4: Stand or sit and turn your arm out so your right hand can touch your right ear. If this is comfortable, try going further behind your head. Hold 5 seconds. Perform 5 times.
Touch Side Pocket/Small of Back – PHOTO 5: Stand or sit and turn your arm in so your right hand can touch your right pocket. If this is comfortable, try going further behind the small of your back or to the back pocket. Hold 5 seconds. Perform 5 times.
Pinch Shoulder Blades Together – PHOTO 6: Stand or sit and pinch your shoulder blades together as if rowing a boat. Hold 5 seconds. Perform 5 times.



Contributions: Gary Mattingly, PT, PhD, Professor Emeritus, University of Scranton, Physical Therapy Department.
Read Dr. Mackarey’s Health & Exercise Forum – every Monday in the Scranton Times-Tribune. Next week will be “Part 3 - shoulder exercises”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at The Commonwealth Medical College.
Part 1 OF 3
The shoulder, working as a ball and socket, is most flexible joint in the human body. It is comprised of two separate joints, the union between the glenoid fossa, (the socket at the end of the scapula or shoulder blade, and the ball at the end top of the humerus, or upper arm bone. The second articulation at the shoulder involves the acromioclavicular joint that connects your scapula to your collar bone. While it is held together by various ligaments, the muscles of the shoulder, namely the rotator cuff, generate the force that allows it to move in multiple directions. The flexibility of the shoulder is thought to be an evolutional advancement as it permits the upper arm to place the hand, and more importantly, the opposing thumbs, in uncountable positions, allowing humans to function at a higher level than other mammals. The ability to paint, draw, play musical instruments, cook, clean, be creative, build, cultivate food, etc. are all directly related to the beautiful and complex cooperative effort between the shoulder, arm and hand.
When the shoulder is compromised by loss of motion or strength, so too is the function of the arm and hand. It becomes difficult to dress, groom, work, play sports, etc. Therefore, it is imperative that we maintain shoulder health through range of motion and strength exercises. However, it is equally important that we exercise in a manner that does not compromise the integrity of shoulder motion or strength. With this in mind, this series of 3 columns will present a list of common shoulder injuries and exercises to maintain or regain range of motion and strength without compromising the joint and muscles.
The most common problems in the shoulder joint include:
Arthritis – inflammation and degeneration of the ends of the bones that form the joint either caused by trauma such as falling of the shoulder or due to a disease such as osteoarthritis or rheumatoid arthritis.
Shoulder Dislocation/Subluxation – when the bones “slide out of position” either caused by trauma or a genetic predisposition.
Torn Rotator Cuff – the rotator cuff is made up of muscles which hold the joint together. A rotator cuff can become torn due to trauma such as falling on the shoulder or following wear and tear from years of overhead activities. Rotator cuff tears are common both in athletes and in the older population.
Impingement – when one or more of the rotator cuff muscles gets pinched between two bones. This is very common and very painful especially when you attempt to raise your hand over your head.
Bursitis – inflammation of a fluid filled sack that tries to protect the shoulder from impingement.
Frozen Shoulder – when the connective tissue that holds the shoulder together becomes too tight. This limits the shoulder‘s freedom of movement. If you have shoulder pain from trauma, tendonitis, or bursitis and the arm is protected at your side for an extended period of time, which allows it to tighten and lose the ability to raise your shoulder. This is more common in middle-aged females, and diabetics.
This is just a partial list of some of the more common problems, which can result in shoulder pain. All of these conditions are uniquely different and need to be treated differently. Some of these conditions respond well to oral medications, others to injection, others to physical therapy and still others may need surgery.
If you have shoulder pain that lasts for more than three days or you notice that you cannot raise your hand over your head, you need to see either your family doctor or an orthopedic surgeon.
Many people have a tendency to at first ignore the problem shoulder thinking that it will get better on its own. This rarely happens. With many shoulder problems the condition just gets worse with time. The longer one waits the greater the chance for greater complications. The sooner one gets medical intervention the quicker the recovery. The bottom line is …DON’T IGNORE SHOULDER PAIN!
If shoulder pain persists, see your physician. However, while waiting for your appointment? There are things that you can do:
Contributions: Gary Mattingly, PT, PhD, Professor Emeritus, University of Scranton, Physical Therapy Department.
