
Michael Morgan, MD3
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
This Holiday Season Give the Gift of Life! Register to be an organ donor
Organ Donation – and ties to NEPA: Part 2 of 2
GCSOM GUEST AUTHOR:
Michael Morgan is a 3rd year medical student at Geisinger Commonwealth School of Medicine. He attended Scranton Prep and graduated Magna Cum Laude from the University of Pittsburgh earning a Bachelor of Science in Finance with minors in Chemistry and Economics. Although he is exploring all future options in clinical rotations, he is currently interested in pursuing a career in surgery or anesthesia. He plans on practicing in the Scranton area upon the completion of his training. Interests include relaxing with family and friends, traveling, and clinical research.
Mike is a member of the Cody Barrasse Memorial Foundation, American Medical Association and American College of Emergency Physicians.
This is the season of giving. Finding the right gift in a land of plenty can be challenging for those fortunate enough to be well-fed and clothed. While there may be many wants and needs we have this holiday season, consider a different kind of gift...GIVE THE GIFT OF LIFE! BECOME AN ORGAN DONOR!
Last week we briefly reviewed the history of organ donation and its local ties to NEPA. Because he was a donor, Cody Barrasse forever changed the lives of nine strangers and their families. Cody, a Penn State student and Scranton Prep alum, tragically passed away following a head injury sustained after being struck by a car as a pedestrian in Pittsburgh in 2013. Cody’s legacy lives on through those who were fortunate enough to have known him and uniquely through those who had received his vital organs. Therefore, the importance of organ donation may vary significantly based one’s personal experience and belief system. For a variety of reasons, some are advocates and some are against. For others, the thought of organ donation is just another question in between them and the door at the Department of Motor Vehicles. In reality, it is a significant life altering decision that can be potentially experienced through someone else, in a positive way!
In 1968, the Uniform Anatomical Gift Act established the Uniform Donor Card as a legal document for anyone 18 years or older to legally donate his or her organs upon death. Despite nearly 50 years of medical triumphs, the concept of organ donation still carries a multitude of myths and misconceptions. It can be a taboo topic. Some believe that the label ‘organ donor’ on an ID means that in an emergent situation, a patient will receive subpar care so that doctors can harvest their organs. This is completely false. Upon taking the Hippocratic Oath at medical school graduation, the patient’s wellbeing is reaffirmed as the physician’s number one priority. Medical personnel will exhaust every avenue in order to save a patient’s life. The medical team working in the emergency room is entirely separate from the group of doctors involved in recovering organs and tissues. The conversation of organ donor status begins only when death is declared and it is confirmed that nothing else can be done for the patient. By dispelling some of the most common misconceptions and by making credible resources available, the hope is that informed decisions can be made and that others can be positively impacted when the unexpected strikes. Here are some of the more common questions surrounding organ donation today:
1. Does organ donation change the appearance of my body? Will I still be able to have a traditional viewing and funeral?
Organ and tissue donation does not disfigure the body. The procedure to preserve and harvest organs is a timely process, it does not interfere with funeral arrangements.
2. Am I too old to register to become an organ donor?
There is no age limit for donation. A potential donor’s organs are evaluated at the time of death to determine their suitability for donation. Anyone interested in becoming an organ donor should indicate their wish on their driver’s license and inform their family that they wish to donate.
3. Do rich and famous people get organs first?
No. The United Network for Organ Sharing (UNOS) matches organs and recipients by weight, height, blood type, followed by medical urgency and time on the waiting list.
4. Is organ donation approved by my religion?
Organ and tissue donation is approved by all major religions in the United States. For many, it is considered a gift – a final act of charity. However, specific concerns or questions should be addressed with your religious advisor.
5. Can I sell my organs?
No, not really. The National Organ Transplant Act (Public Law 98-507) made the buying and selling of organs and tissues illegal in 1984. However, the selling of plasma, a component of blood, is legal. Blood is technically an organ so I’d presume that selling one of its components counts. In Pennsylvania, is legal to “donate” plasma up to two times a week. Each time a blood bank will pay approximately $30 for the specimen.
Medical Contributor: Linda Barrasse, MD
For more information or to learn how you can become more involved in organ donation, please visit http://codybarrassefoundation.com/organ-donation/
Read Part 1 of this series here.
Sources:
http://www.liveonny.org/all-about-transplantation/organ-transplant-history/http://www.donatelifepa.com/register
http://www.donatingplasma.org/donation/donor-faq
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commowealth Medical College).
Michael Morgan, MD3
Register to be an organ donor, Organ Donation – and ties to NEPA: Part 1 of 2
GCSOM GUEST AUTHOR: Michael Morgan, MD3
Michael Morgan is a 3rd year medical student at Geisinger Commonwealth School of Medicine. He attended Scranton Prep and graduated Magna Cum Laude from the University of Pittsburgh earning a Bachelor of Science in Finance with minors in Chemistry and Economics. Although he is exploring all future options in clinical rotations, he is currently interested in pursuing a career in surgery or anesthesia. He plans on practicing in the Scranton area upon the completion of his training. Interests include relaxing with family and friends, traveling, and clinical research.
Mike is a member of the Cody Barrasse Memorial Foundation, American Medical Association and American College of Emergency Physicians.
This is the season of giving. Finding the right gift in a land of plenty can be challenging for those fortunate enough to be well-fed and clothed. While there may be many wants and needs we have this holiday season, consider a different kind of gift...GIVE THE GIFT OF LIFE! BECOME AN ORGAN DONOR!
On December 23rd, 1954 the term ‘modern medicine’ was redefined. At Brigham Hospital in Boston, Massachusetts, Dr. Joseph Murray and his team performed the first successful living-related kidney transplant on identical twin brothers. Eight years later the same team was able to successfully transplant a kidney from a deceased donor. For the very first time medically, there was life after death. At a rapid pace across the country, brazen surgeons and their colleagues altered the medical landscape by performing heart, lung, and liver transplants. Necessary complimentary immunosuppressive therapies were developed along the way. These medicines extended the lifespan of existing transplants, and also led way to other, more aggressive procedures. Over time, surgical techniques were refined and more lifesaving drugs were discovered. This data was then optimized and shared among providers to establish a novel lifesaving procedure that would go on to affect millions of patients and their families – organ transplantation.
Locally, the limitless potential of organ transplantation was experienced following the untimely death of Cody Barrasse in 2013. Cody was just 22 years old when he died following a head injury that he sustained after being struck by a car as a pedestrian while visiting friends in Pittsburgh. Cody had a unique and special spirit that is actively celebrated by all who knew him. However, the patients who received his vital organs truly understand the gravity of what it means to be an organ donor. Nine different people and their families can celebrate life today because of one selfless decision made by Cody. He gave 9 organs and tissues to 7 different people including: a heart to a nine year old, part of his liver to an 18 month old and the other part to a middle-age woman, one kidney to a women and the other kidney, along with his pancreas, to a 12 year old. He also gave his cornea and skin to improve the lives of complete strangers. There is no price tag for the bride who was able to have her father walk her down the aisle because he had received Cody’s lungs. The kindergartener who received part of his liver doesn’t remember the lifesaving transplant she had at 18 months, but her family sure does. Because of the incredible advancements in organ transplantation, diagnoses that once meant certain death now carry a glimmer of hope. Positives can be created out of tragedy with proper planning. Making the decision to become an organ donor, like Cody, can be the first step. For more information or to learn how you can become more involved in organ donation, please visit http://codybarrassefoundation.com/organ-donation/
For many, the thought of being an organ donor is a difficult concept to grasp. It can be an uncomfortable and unsettling conversation. There are many myths and misconceptions that surround organ donation which can make one’s decision even more perplexing. By dispelling some of the most common myths, and by making credible resources available, the hope is that the most informed decisions can be made and that others can be positively impacted when the unexpected strikes. Next week’s column will address questions that are asked by people every day like: Does my decision to become an organ donor affect the quality of my medical care? (It doesn’t.)
Medical Contributor: Linda Barrasse, MD
For more information or to learn how you can become more involved in organ donation, please visit http://codybarrassefoundation.com/organ-donation/
Sources:
http://www.liveonny.org/all-about-transplantation/organ-transplant-history/
http://www.donatelifepa.com/register
http://www.donatingplasma.org/donation/donor-faq
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Organ Donation – Part 2 of 2.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commowealth Medical College).
 Holiday shopping is stressful to your body as well as your wallet. Driving from store to store, getting in and out of the car, bundled in a sweater and winter coat, the expert shopper carries package after package from the store, to the car, over and over again. Six, eight, or ten hours later, the shopper arrives home exhausted, only to realize that 15, or 20 packages must be carried from the car into the house. This dilemma is compounded by the fact that the rain turned to sleet, and the sleet to snow. Travel by car and foot are treacherous. You are slipping and sliding all the way from the car to the house while carrying multiple packages of various sizes and shapes. The shopping bags get wet and tear, forcing you to tilt your body as you carry the packages. Of course, no one is home to help you unload the car and you make the trip several times alone. You get into the house exhausted and crash onto the couch. You fall asleep slouched and slumped in an overstuffed pillow chair. Hours later you wake up with a stiff neck and lower back pain. You wonder what happened to your neck and back. Consider the following:
Holiday shopping is stressful to your body as well as your wallet. Driving from store to store, getting in and out of the car, bundled in a sweater and winter coat, the expert shopper carries package after package from the store, to the car, over and over again. Six, eight, or ten hours later, the shopper arrives home exhausted, only to realize that 15, or 20 packages must be carried from the car into the house. This dilemma is compounded by the fact that the rain turned to sleet, and the sleet to snow. Travel by car and foot are treacherous. You are slipping and sliding all the way from the car to the house while carrying multiple packages of various sizes and shapes. The shopping bags get wet and tear, forcing you to tilt your body as you carry the packages. Of course, no one is home to help you unload the car and you make the trip several times alone. You get into the house exhausted and crash onto the couch. You fall asleep slouched and slumped in an overstuffed pillow chair. Hours later you wake up with a stiff neck and lower back pain. You wonder what happened to your neck and back. Consider the following:
Plan Ahead: It is very stressful on your spirit, wallet and back to do all of your shopping in the three weeks available after Thanksgiving. Even though we dislike “rushing” past Thanksgiving to the next holiday, try to begin holiday shopping in before
Use the Internet: Supporting local businesses is important. However, Internet shopping can save you lots of wear and tear. Sometimes, you can even get a gift wrapped.
Gift Certificates: While gift certificates may be impersonal, they are easy, convenient and can also be purchased over the internet.
Perform Stretching Exercises: Chin Tucks, Shoulder Blade Pinch, Back Extension. Stretch intermittently throughout the shopping day…try the three exercises below, gently, slowly, hold 3 seconds and relax, repeat 5 times.
Photo 1: Chin Tucks – Bring head over shoulders
Photo 2: Shoulder Blade Pinch – Pinch shoulder blades together (row the boat)
Photo 3: Back Extension – Stretch backwards



Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
ACHILLIES TENDON RUPTURE: Part 2 of 2
(read Part 1 here)
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to warm-up and exercise during the winter months. A little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears. The Achilles tendon is one of the more common tendons torn.
This is the second of two columns on Achilles tendon rupture. Last week, I discussed the definition, sign and symptoms of the problem. This week will present examination, treatment and outcomes.
A thorough history and physical exam is the first and best method to assess the extent of the injury and determine accurate diagnosis. While a complete tear is relatively easy to determine, a partial or incomplete tear is less clear. Ultrasound and MRI are valuable tests in these cases. X-rays are not usually used and will not show tendon damage.
Initial First Aide Treatment
Early Treatment - Conservative
Surgery
Consultation with an orthopedic or podiatric surgeon will determine the best treatment option for you. When conservative measures fail and for tendons completely torn, surgical intervention is usually considered to be the best option with a lower incidence of re-rupture. Surgery involves reattaching the two torn ends. In some instances, a graft using another tendon is required. A cast or walking boot is used post-operatively for 6-8 weeks followed by physical therapy.
Most people return to close to normal activity with proper management. In the competitive athlete or very active individual, surgery offers the best outcome for those with significant or complete tears, to withstand the rigors of sports. Also, an aggressive rehabilitation program will expedite the process and improve the outcome. Walking with full weight on the leg after surgery usually begins at 6 -8 weeks and often requires a heel lift to protect the tendon. Advanced exercises often begin at 12 weeks and running and jumping 5-6 months. While a small bump remains on the tendon at the site of surgery, the tendon is well healed at 6 months and re-injury does not usually occur.
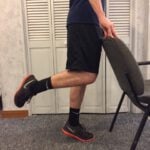
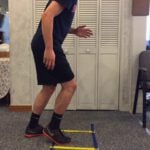
Prevention of muscle and tendon tears is critical for healthy longevity in sports and activities. In addition to the Achilles tendon, the tendons of the quadriceps (knee) and rotator cuff (shoulder) are also vulnerable. A comprehensive prevention program includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions. Also, utilizing interval training, eccentric exercise (lowering body weight slowly against gravity – Photo 1) and proprioceptive and agility drills are essential (Photos 2 & 3).
PHOTO 1a & 1b: Eccentric Lowering and Lengthening: for the Achilles tendon during exercise. Beginning on the ball of both feet (1a), bend the strong knee to shift the weight onto the weak leg (1b). Slowly lowering the ankle/heel to the ground over 5-6 seconds. Repeat.
PHOTO 2: Proprioceptive Training: for the Achillies tendon. Standing on a Bosu Ball while exercising the upper body (for example, biceps curls, shrugs, rows, lats) while maintaining balance on the ball.
PHOTO 3: Agility Drills: for the Achilles tendon involves stepping through a “gait ladder” in various patterns and at various speeds.


MODEL: Ben Rutledge
Sources: MayoClinic.com; Christopher C Nannini, MD, Northwest Medical Center;Scott H Plantz, MD, Mount Sinai School of Medicine
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
As the days continue to get shorter and temperatures begin a slow steady decline, athletes and exercise enthusiasts will work harder to “fit in” a warm-up before running or other activities during the winter months. But, no matter how limited time is, skipping the warm-up is risky. This time of year, one can expect to feel a little cold and stiff, especially if you are over 40, and therefore a little caution and preparation are in order to avoid muscle/tendon strain, or worse yet, muscle/tendon tears. The Achilles tendon is one of the more common tendons torn. Prevention of muscle tears, including the Achilles tendon includes; gradual introduction to new activities, good overall conditioning, sport specific training, pre-stretch warm-up, stretch, strengthening, proper shoes, clothing, and equipment for the sport and conditions.
A muscle contracts to move bones and joints in the body. The tendon is the fibrous tissue that attaches muscle to bone. Great force is transmitted across a tendon which, in the lower body, can be more than 5 times your body weight. Often, a tendon can become inflamed, irritated, strained or partially torn from improper mechanics or overuse. Although infrequent, occasionally tendons can also snap or rupture. A tendon is more vulnerable to a rupture for several reasons such as a history of repeated injections of steroids into a tendon and use of medications such as corticosteroids and some antibiotics. Certain diseases such as gout, arthritis, diabetes or hyperparathyroidism can contribute to tendon tears. Also, age, obesity and gender are significant risk factors as middle-aged, overweight males are more susceptible to tendon tears. Poor conditioning, improper warm-up and cold temperatures may also contribute to the problem.
Tendon rupture is very painful and debilitating and must not be left untreated. While conservative management is preferred, surgical management is usually required for complete tears. The purpose of this column is to present the signs, symptoms and management of Achilles tendon ruptures.
The Achilles tendon (also called the calcaneal tendon), is a large, strong cordlike band of fibrous tissue in the back of the ankle. The tendon (also called the heel cord) connects the powerful calf muscle to the heel bone (also called the calcaneus). When the calf muscle contracts, (as when you walk on the ball of your foot), the Achilles tendon is tightened, tension is created at the heel and the foot points down like pushing a gas pedal or walking on tip of your toes. This motion is essential for activities such as walking, running, and jumping. A partial tear of the tendon would make these activities weak and painful, while a full tear through the tendon would render these activities impossible.
With age, the Achilles tendon (and other tendons) gets weak, thin, and dehydrated, thus making it prone to inflammation, degeneration, partial tear or rupture. The middle-aged weekend warrior is at greatest risk. A full or complete tear (Achilles tendon rupture) usually occurs about 2 inches above the heel bone and is associated with a sudden burst of activity followed by a quick stop or a quick start or change in direction, as in tennis, racquet ball, and basketball.
In some instances, the tendon can be injured by a violent contraction of calf when you push off forcefully at the same time the knee is locked straight as in a sudden sprint. Other times, the tendon is injured when a sudden and unexpected force occurs as in a trip off a curb or sudden step into a hole or a quick attempt to break a fall.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week: Achilles tendon Part 2 of 2.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.

Branston Allen, MD3
This column is a monthly feature of “Health & Exercise Forum” in association with the students and faculty of Geisinger Commonwealth School of Medicine (formerly The Commonwealth Medical College).
Hunters and Heart Attacks: The Dangers of Buck Fever: Part 2 of 2
Branston Allen, MD3
Branson is a currently a 3rd year medical student at the newly named Geisinger Commonwealth School of Medicine. He is a graduate of Lock Haven University and Shippensburg Area High School. Branson grew up in Shippensburg as an avid outdoorsman and enjoys activities ranging from hunting to fishing to camping.
As the temperature drops and the leaves fall, nearly one million Pennsylvanians take up their trusty deer rifles and plunge into the woods with hopes of dragging out a prized white-tailed deer. Historically, rifle season commences on the first Monday after Thanksgiving, which will be November 27th this year. Hunters and loved ones often worry about potentially fatal misfortunates that can occur while secluded in the forest. These concerns range from stray bullets to tree stand falls. However, according to many experts, a heart attack is up to three times more likely to claim a hunter’s life than an errant bullet.
As a third year medical student, I’ve actually already encountered a local gentleman whose heart carries the scar of a heart attack he experienced while hunting. To protect his identity, I’ll refer to him as John. John – “November was always my favorite month of the year. Thanksgiving is a nice holiday and it’s great to see family. But the best part about it is deer season”. John is a 68 year old, recent retiree who was born and raised in Luzerne County. Like a lot of NEPA residents, he probably eats a few too many pierogis and drinks a few too many beers, but otherwise is pretty healthy. He worked most of his life in a local warehouse, and always requested off for the first 3 days of deer season. Last deer season was almost John’s last. “It was the second day of the season and I finally managed to get a clean shot at a nice sized doe. I was dragging her out whenever I got this massive pain across my chest. I was sweating like crazy and it felt like an elephant was sitting on my chest. After I few minutes, I got really nervous and called my wife. She told me to call 911” – John. Fortunately for John, his story had a happy ending. “The doc told me I had about a 99% block of a vessel in my heart that is called ‘the widow-maker’ and that I experienced a mild heart attack. Thankfully, they were able to fix me up with surgery, and I feel like lucky to still be here today”.
Most people know a man like John and these are the type of people who we worry most about having heart attacks while they are hunting. The American Heart Association has identified men over the age of 45 and females above the age of 55 as the population most likely to suffer from cardiovascular disease. According to the Pennsylvania Game Commission, the majority of hunters are males of the age of 45, and these individuals are often overweight and don’t get much exercise throughout the year. When deer season comes, they’re putting strain on their muscles and heart in a way that their body isn’t used to dealing with. This increased demand on their hearts causes their heart rates to soar and can produce some of the tell-tale signs of heart disease. These include chest pain, arm pain or numbness, and shortness of breath. Additional risk factors such as high blood pressure, high cholesterol, obesity, and a sedentary lifestyle also increase one’s chances of suffering a heart attack.
What makes hunting especially scary is it stresses your body in ways everyday life doesn’t. Hunters must contend with the elements and temperatures associated with late November in Pennsylvania, the adrenaline surges associated with spotting a deer, and the daunting physical task of dragging 120+ pound deer out of woods if they shoot true. Any of these situations individually is capable of sending heart rates soaring. Complicating the hike into the woods on uneven terrain is the added weight of a gun, ammunition and other supplies. Also, trekking through mud or snow increases the physical demands exponentially. A research study out of Beaumont Hospital in Michigan found that the majority of hunters experience circumstances in which their heart rates exceed 85% of their maximum heart for sustained periods of time, which greatly increases the risk of a sedentary, unfit individual of sustaining a heart attack. Furthermore, hunters were more likely to demonstrate heart ischemia and arrhythmias during hunting than they were during a usual stress test with a treadmill. Arrhythmias are usually the cause of death when somebody experiences a heart attack, which makes these findings especially troublesome.
So what can you do to keep yourself or your loved one safe during hunting season? First and foremost, if you experience any chest pain or shortness of breath on exertion, see your doctor immediately. Secondly, if you are a man over the age of 45 and have risk factors for heart disease such as hypertension, high cholesterol, diabetes, obesity, and/or live a sedentary lifestyle, talk to your doctor before you head out into the woods this year to make sure your heart can take all of the stress associated with hunting. Make sure that somebody knows where you’re at and can call for help if they don’t hear from you. If you have trouble walking or have risk factors for a heart attack, carry a cell phone with you and try to hunt near a place with vehicle access. Finally, just be smart and exercise caution while hunting. Listen to your body. Take as many breaks as you need while you are hiking into or out of your favorite hunting spot. If you manage to harvest a deer, take your time dragging it out of the woods. Drag, rest, and drag again. Better yet, call in backup and get some help with the drag, especially if you are a more seasoned hunter. You have earned the right to relax and employ the help of younger hunters to assist you. By doing this, you can ensure that this year’s deer won’t be your last.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com.
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine (formerly The Commowealth Medical College).
While I am not a hunter, I am an avid outdoors person with great passion for mountain biking, kayaking, whitewater rafting, hiking and mountain climbing in our state and national parks. With this in mind, I offer hunter safety tips based on the knowledge of experts in the field and offer health safety associated with outdoor activity based on my expertise as a health care provider. Good luck and be safe!
Next week: Read Hunting Safety - Part 2 by GCSOM 3rd Year Medical Student and Avid Hunter, Branston Allen MD3
Next week: Read Hunting Safety - Part 2 by GCSOM 3rd Year Medical Student and Avid Hunter, Branston Allen MD3
Sources: www.pgc.state.pa.us
Visit your doctor regularly and listen to your body.
Keep moving, eat healthy foods, exercise regularly, and live long and well!
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum” in the Scranton Times-Tribune.
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at Geisinger Commonwealth School of Medicine.
November is National Alzheimer’s Disease Awareness Month. It is appropriate that it is also National Family Caregivers Month, considering the fact that many people afflicted with Alzheimer’s are physically fairly well and often rely on caregivers. It would be very unusual to find a person whose life has not been affected by someone with Alzheimer’s disease (AD). AD is one form of dementia. It is sometimes referred to as Senile dementia/Alzheimer’s type (SDAT). Currently, more than 4 million people in the USA have AD. Approximately 10% of all people over 70 have significant memory deficits. The number doubles each decade after 70. The risk increases with age and family history for the disease.
AD is a progressive degenerative disease of the brain that affects memory and thought process. Memory impairment is the hallmark of this disease. Also, those suffering from AD present changes with the following: language, decision-making, judgment, attention, and other personality or aspects of mental function. AD progresses differently in each case.
Two types of AD have been identified, early onset and late onset. In early onset, symptoms appear before the age of 60 and progresses very rapidly. It accounts for 5-10% of all cases. Autosomal dominant inherited mutations have been found in early onset AD.
The cause of AD is not completely understood, however, most experts agree that both genetic and environmental factors are involved. It is important to rule out other medical causes before a final diagnosis of AD can be made. Only a post-mortem microscopic examination of brain tissue can confirm the diagnosis. Structural and chemical parts of the brain disconnect as the brain tissue shows twisted fragments of protein that clogs up the nerve. Clusters of dead and dying nerve cells block the transmission of information and communication from one nerve cell to the next. AD causes a disconnection of areas of the brain that normally work together.
The Greater Boston Physicians for Social Responsibility and the Science and Environmental Health Network offer the following guidelines to
Reduce the Risk of Developing AD:
Source: The HealthCentralNetwork, Inc
Read Dr. Mackarey’s Health & Exercise Forum – Every Monday in the Scranton Times-Tribune. This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com.
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
FLU MYTHS: Part 2 of 2
At this time every year, patients come to our office with questions and concerns about the flu shot. The most frequently asked questions is, “Can the flu shot give me the flu?” As you are about to learn, the answer is NO! In fact, in well-designed scientific studies, where some people get flu shots and others get salt-water shots, the only difference in symptoms was increased soreness in the arm and redness at the injection site among people who got the flu shot. There were no differences in terms of body aches, fever, cough, runny nose or sore throat.
Common Flu Myths:
1) You can catch the flu from flu vaccine: While many people may feel a bit lousy after a flu shot, it is not Influenza. There is a certain amount of normal and expected reaction that occurs after any vaccination. This is the body responding appropriately to the vaccine and building antibodies to prevent future infection. Of the 2 types of flu vaccine, neither injects the influenza virus that is seen in the environment. The live attenuated vaccine contains weakened virus designed to stimulate the immune system with virus strains that are expected to be in the community during influenza season, but in a much weakened form. While people with impaired immune systems should not receive this vaccine, it is safe in individuals with normal immune systems. The inactivated vaccine contains no infectious virus; it is inactivated. As such, these types of vaccines do not cause influenza and are able to stimulate a protective immune response.
2) It’s too late to get the flu shot this year: Influenza typically peaks after the New Year and runs into the spring in the Northern Hemisphere. Receiving vaccine in December will still provide a good deal of protection. However, it’s a good idea to get vaccinated as soon as the vaccine is available in early fall.
3) Healthy people don’t need to get vaccinated: While individuals with chronic illnesses and the elderly are at higher risk for influenza, healthy people can get sick as well. Additionally, those who are healthy and unvaccinated can spread the disease to those around them if they do get sick with influenza. Healthy people should get vaccinated.
4) You don’t need to get a flu shot every year: Due to the potential for strain change (the specific types of influenza virus circulating in a particular year) vaccination with the most current vaccine is necessary. Additionally, an individual’s immune response, and thus protection, may not last long enough to protect over two seasons even if the strains are unchanged. To be certain you have the maximum protection, an annual flu shot is recommended.
5) Once I have the flu I don’t need to get vaccinated: While having a true case of influenza may protect you from that strain in that particular year, there are many different types of influenza in circulation. You will still be susceptible to any of the other strains despite your illness. You should still be vaccinated. However, vaccination should occur when you are well.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!”
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com. Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
FLU MYTHS: Part 1 of 2
At this time every year, patients come to our office with questions and concerns about the flu shot. In an attempt to educate the public and dispel any fears or misconceptions,
Influenza has a long recorded history in medicine. It was first mentioned by Hippocrates in 412 BC. The first epidemic was reported in 1510 and the first pandemic in 1580. There have been 32 pandemics since 1580 with the most recent being in 2009 with the well known H1N1 virus. Influenza remains a serious illness with 40,000 deaths and 200,000 hospitalizations annually in the US. It’s estimated that between 5-20% of the US population will get Influenza each season with an estimated direct cost for care of 10 billion dollars.
Clinical symptoms:
Haemophilus Influenzae virus infects the respiratory epithelium or lining in the lungs. Onset of symptoms can be sudden with high fever, fatigue and muscle aches. Cough is usually present, is non-productive and can be severe. Symptoms can last for several days with fatigue lasting for 2-3 weeks. During the acute phase of illness, patients are at higher risk for secondary bacterial infections such as pneumonia.
Diagnosis:
Definitive diagnosis of influenza is made with a nasal swab and culture. The swab is obtained by placing a small probe into the nose and obtaining material from deep inside. This material is then sent to a lab and cultured in the hopes of identifying the causative agent
Treatment:
There are effective antiviral medicines for the treatment of influenza. They are best used at first sign of disease and may shorten the period of illness or decrease disease severity. Other medical interventions are supportive. Treating any underlying symptoms such as muscle pain and promptly treating any complications such as bacterial pneumonia. Antivirals can also be used to prevent influenza and are used when exposure to someone with influenza is known and unavoidable such as in nursing home patients.
Populations at Risk:
Influenza can strike any age group and both males and females are at risk. However, the elderly, the very young and those with underlying medical conditions are most at risk. Those over the age of 65, those with underlying lung disease, heart disease, diabetes, cancer, kidney disease or those with impaired immune function are at particularly high risk. Additionally, those in nursing homes and chronic care facilities are also at increased risk.
Vaccination:
Vaccination is recommended for those 6 months and older. There are 2 main types of vaccines available: live attenuated (weakened) and inactivated. Because the live attenuated vaccine carries very small risks of disease in certain high risk groups (ie: impaired immune function), the live attenuated vaccine is only recommended for use in healthy adults under the age of 50. The inactivated vaccine can be administered to anyone without previous reaction or known allergy.
Vaccine Effectiveness:
The effectiveness of the influenza vaccine depends on a few factors. One is the match of the vaccine to circulating strains in the community. When the strain predicted to be circulating and thus present in the vaccine is a good match, the vaccine can provide protection in greater than 75% of those who receive it. Another important factor in vaccine effectiveness is the individuals’ immune response. Those over the age of 65 have been shown to have a slightly lower immune response to the vaccine. It is a function of general immune responsiveness and not due to the vaccine itself. Clearly, however, those individuals who receive the vaccine are much more likely to be protected than those who remain unvaccinated.
The Future:
Vaccine manufacturers continue to work on improving the influenza vaccine with the aim of providing broader coverage to a greater number of people. For example, there is a great deal of work being done on developing a Universal Flu Vaccine; one that identifies commonality among the many strains and will provide broader protection without the concern of strain match. A recently available high dose vaccine for those over the age of 65 was developed in the hope that a higher dose would provide those individuals in this age range a better and more consistent immune response than standard dose vaccine.
Visit your doctor regularly and listen to your body.
NEXT MONDAY – Read Dr. Paul J. Mackarey “Health & Exercise Forum!” Next Week: The Flu – Part 2
This article is not intended as a substitute for medical treatment. If you have questions related to your medical condition, please contact your family physician. For further inquires related to this topic email: drpmackarey@msn.com
Paul J. Mackarey PT, DHSc, OCS is a Doctor in Health Sciences specializing in orthopaedic and sports physical therapy. Dr. Mackarey is in private practice and is an associate professor of clinical medicine at GCSOM.
